Document Type : Review Article
Keywords
Subjects
Introduction
Multiple sclerosis (MS) is an inflammatory and demyelinating disease of the central nervous system (CNS) (1). In certain conditions such as systemic inflammation pro-inflammatory cytokines could be released which will affect the neural activity and worsen the damage to the CNS in the presence of a neurodegenerative disease such as MS (2, 3). It has been observed that the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) which is responsible for the COVID-19 infection, can trigger an immune response by activating the innate and adaptive immune system and the overproduction of inflammatory cytokines (4). Microbial infections can induce immune responses not only for their own specific antigen (Ag), but can also trigger responses against self-Ags which results in inflammation (5, 6). Previous studies have suggested a strong relationship between viral infections and clinical expression of MS (7-10).
The immune system dysregulation which leads to organ damage in autoimmune disease can also be seen in COVID-19 (11). Reports have shown that Guillain-Barre syndrome, autoimmune thyroid disease, and detection of autoantibodies in COVID-19 infected individuals are some of the autoimmune complications associated with COVID-19 (12).
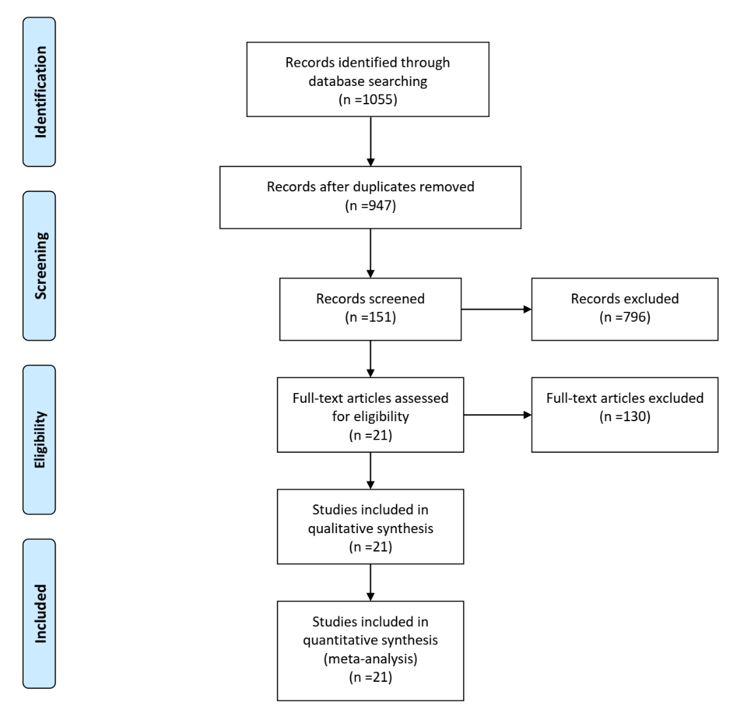
Figure 1. From: Moher D, Liberati A, Tetzlaff J, Altman DG, The PRISMA Group (2009). Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med 6(6): e1000097. doi:10.1371/journal.pmed1000097.
Results about the relapse rate of MS following COVID-19 infection varies among studies. A number of studies have suggested that COVID-19 infection could exacerbate MS symptoms and promote relapse (13, 14). For example, in a case report by Paolo et al. a patient with reduced visual acuity and demyelinating lesions in MRI of the CNS following COVID-19 infection was reported (15) while Etemadifar et al. found that COVID-19 infection showed no association with increased risk of relapse (16).
COVID-19 vaccination is the main strategy to prevent COVID infection, especially in at-risk people such as MS patients (17). Numerous studies and case reports have demonstrated the presence of autoantibodies and autoimmune complications like neuropathy and demyelination following vaccination (18, 19).
Since there has been evidence of acute MS relapse following vaccination concerns raised about the safety of different COVID vaccines among MS patients (20, 21). A recent study by Fragoso et al. has observed increased relapse rate and new lesions on magnetic resonance imaging (MRI) of MS patients following vaccination (22). Based on these findings we designed this systematic review and meta-analysis to investigate the prevalence of relapses in MS patients following COVID-19 infection and vaccination.
Methods
The meta-analysis was conducted following Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guideline (23).
Search strategy
We systematically searched four databases including, PubMed, web of science, Scopus, and Embase in January 2023. For our search strategy we used the following terms: (Multiple sclerosis) AND (COVID-19 OR SARS-COV-2 OR corona virus OR coronavirus disease OR 2019-nCoV Disease) AND (Vaccination OR Vaccine OR immunization).
Inclusion criteria
we included any cohort, case-control or cross-sectional study about the relapse rate in MS patients following either COVID infection or COVID vaccination.
Exclusion criteria
The non-English papers, studies investigating the vaccination for other virus in MS patients, review and case report articles were excluded.
Study selection
Two reviewers (MB, MM) screened the articles in a two-step process. First, reviewers screened title and abstracts of the retrieved articles according to the inclusion criteria and in the second step the same reviewers assessed the full text of the chosen articles based on the predefined criteria.
Quality assessments
The quality of the included articles was assessed using the Newcastle-Ottawa Scale (NOS). Risk of bias of studies assessed in the selection, comparability, and exposure with the highest possible score of 8.
|
Table 1. |
||||||||||||||
|
Author |
Year |
Continent |
Region |
study design |
mean ag(SD) |
total patients |
male patients |
type of MS |
disease duration |
follow-up time |
base EDSS |
acute relapses |
name of vaccine |
|
|
Achiron et al. |
2021 |
Asia |
Israel |
Cohort |
NM |
555 |
342 |
RIS:7, CIS:39, RRMS:694,SPMS:162, PPMS:88 |
15.2(median |
38 days 1st dose, 20 days 2nd dose |
8 by 1st dose, 5 by 2nd dose |
Pfizer/BioNTech |
||
|
Sahraian et al. |
2021 |
Asia |
Iran |
Observational study |
36.2 |
579 |
130 |
RRMS:442, SPMS:112, PPMS:20 |
NM |
NM |
3 |
5 |
Sinopharm vaccine |
|
|
Philbey et al. |
2021 |
Europe |
England |
Observational study |
50 |
33 |
14 |
RRMS:19, SPMS:9, PPMS:5 |
NM |
7 days |
4 |
0 |
AstraZeneca:29, BioNTech/Pfizer:4 |
|
|
Philbey et al. |
2022 |
Europe |
England |
Cohort |
47.4 |
193 |
66 |
RRMS:147, PPMS:16, SPMS:30 |
12(median) |
21 days 1st dose, 49 days 2nd dose |
3.5 |
4 |
Pfizer/BioNTech:49, AstraZeneca:144 |
|
|
Alonso et al. |
2021 |
South america |
Latin america |
Cross-sectional study |
41.5 |
393 |
69 |
RRMS:310 ,SPMS:12 ,PPMS:28, Unknown to participant:43 |
8.5±8.2 |
NM |
4 |
5 |
Pfizer/BioNTech:49, Moderna:2, CoronaVac/Sinovac:80, Sinopharm:70, Sputnik V:116, Covishield:33, Oxford AztraZeneca:42, Johnson & Johnson:1 |
|
|
Maniscalco et al. |
2022 |
Europe |
Italy |
retrospective observational study |
45.9 |
310 |
115 |
RRMS:270 |
11.8 |
20 days |
first dose:3 |
Pfizer/BioNTech |
||
|
Kong et al. |
2022 |
Asia |
China |
cohort |
35.85±9.38 |
78 |
31 |
RRMS |
4.59 |
9.4 months |
NM |
4 |
inactivated SARS-CoV-2 vaccine |
|
|
Czarnowska et al. |
2022 |
eurpe |
poland |
cohort |
42.61 |
2261 |
667 |
RRMS:2149 |
9.48±6.35 |
NM |
2.4±1.45 |
99 |
Pfizer/BioNTech:1684 |
|
|
Di Filippo et al. |
2021 |
europe |
Italy |
cohort |
42.7±10.8 |
324 |
82 |
RRMS:303 |
11.9±8.5 |
2 months |
2.1±1.5 |
7 |
Pfizer/BioNTech |
|
|
Kavosh et al. |
2022 |
Asia |
Iran |
cross-sectional |
40.45 ± 9.74 |
1538 |
387 |
NM |
10.38 ± 6.81 |
NM |
2.06 ± 3.16 |
first dose:10 |
Sinopharm |
|
|
Frahm et al. |
2022 |
Europe |
germany |
longitudinal observational study |
45.7 ±11.4 |
2346 |
503 |
RRMS:1749 |
NM |
2 months |
NM |
first dose:79 |
BioNTech/ Pfizer, Moderna, AstraZeneca, Johnson&Johnson |
|
|
Alster et al. |
2022 |
Asia |
Israel |
Cohort |
NM |
211 |
80 |
CIS:7 |
16.65 years median |
66 days |
NM |
7 |
Pfizer/BioNTech |
|
|
Czarnowska et al. |
2022 |
Europe |
poland |
Cohort |
41.88 |
1668 |
459 |
RRMS:1585 |
9.44 years |
7 months |
2.36 |
67 |
Pfizer/BioNTech:1215 |
|
|
Ciampi et al. |
2022 |
South america |
chile |
Cohort |
39.7 ± 11.2 |
178 |
57 |
RRMS:152 |
7.4 ± 6.5 |
1 year |
2 |
4 |
Coronavac-Sinovac:123 |
|
|
Alroughani et al. |
2022 |
Asia |
Kuwait |
Cohort |
36.82 + 8.80 |
383 |
136 |
NM |
36.82 + 8.80 |
NM |
3 |
5 |
Pfizer/BioNTech:225 |
|
|
NM, not mentined |
||||||||||||||
Statistical analysis
Analysis was performed using “meta” and “metafor” packages in R 4.2.2. A random effect model was conducted for all analyses considering high heterogeneity between studies. Heterogeneity was assessed using Q, Ƭ2, and I2 statistics. For all metrics overall proportion was calculated (using Freeman-Tukey double arcsine transformation). If enough data was available the difference between dose one and dose two was also investigated.
Results
Study selection
A total of 947 articles were identified via a search in the electronic databases (Figure 1). 151 articles met our inclusion criteria after the first step of screening. After a full-text review, 130 articles were excluded and 21 articles were included in the present meta-analysis. Selected studies are grouped into two groups: acute relapses of MS after COVID infection and COVID vaccination.
Characteristics of included studies and a qualitative summary
The characteristics of included studies are described in Table 1 and Table 2. We identified 21 observational studies with a total of 11546 MS patients. The included studies were conducted in 2021 and 2022 during the COVID pandemic. Overall, 8, 10, and 3 studies were from Europe, Asia, and America, respectively. studies in Table 1 investigated the relapse and adverse events in MS patients vaccinated with different vaccines, either mRNA vaccines or inactivated vaccines. Most patients were vaccinated with the first dose or both first and second doses, however, one study reported the events following administration of the third dose in MS patients. All included studies were determined to be high quality with a mean score of 7.76 for 21 studies (Table 3). The quality of studies assessed using NOS is presented in Supplementary 1.
Meta-analysis
The prevalence of acute relapse following COVID vaccine was 2% (95% CI 2%-3%) (Figure 2) which was lower compared to the prevalence of relapse following COVID infection 7% (95% CI 4%-12%) (Figure2). The prevalence of pseudo relapse (a transient increase in MS symptoms following vaccination) among 4 studies was 5% (95% CI 2%-11%) (Figure 3).
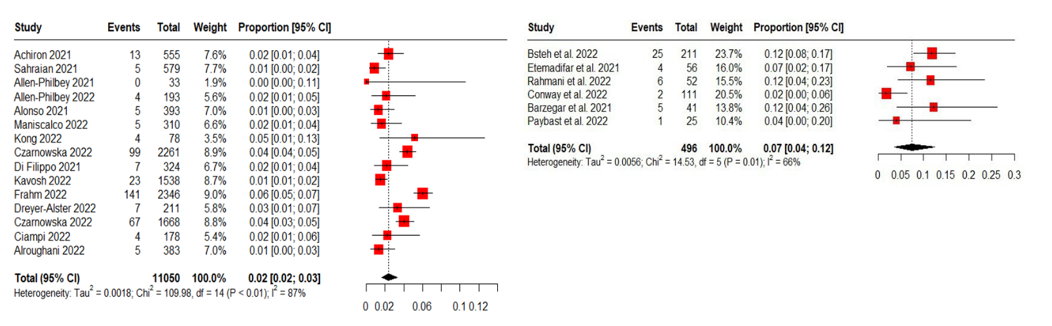
Figure 2. The prevalence of acute relapses following COVID-19 infection (right) and COVID-19 vaccine (left) in MS patients.
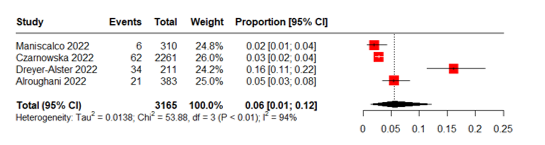
Figure 3. The prevalence of pseudorelapses following vaccination in MS patients.
|
Table 2 |
|||||||||||||||
|
Author |
Year |
Continent |
Region |
study design |
mean ag(SD) |
total patients |
male patients |
type of MS |
MS duration |
follow-up time |
base EDSS |
patients with MRI emhancements |
relapses |
|
|
|
Bsteh et al. |
2022 |
europe |
Austria |
cohort |
42.6 |
211 |
65 |
RRMS:170 |
12.1 |
6 months |
1.5 |
NM |
24 |
|
|
|
SPMS:30 |
|
||||||||||||||
|
PPMS:11 |
|
||||||||||||||
|
Etemadifar et al. |
2021 |
Asia |
Iran |
retrospective cohort |
36.89 ±9.06 |
56 |
15 |
RRMS |
7.76 ±5.07 |
6 months |
1.5 |
NM |
4 |
|
|
|
Rahmani et al. |
2022 |
Asia |
Iran |
case-control |
37.6 ±9.23 |
52 |
13 |
RRMS |
52 months |
6 months |
2.07 ±1.87 |
4 |
6 |
|
|
|
Conway et al. |
2022 |
America |
USA |
retrospective cohort |
49.3±12.2 |
111 |
26 |
RRMS:72 |
13.1± 9.6 |
17.1 ±13.6 |
2.5 |
5 |
2 |
|
|
|
CIS:2 |
|
||||||||||||||
|
SPMS:21 |
|
||||||||||||||
|
PPMS:8 |
|
||||||||||||||
|
Barzegar et al. |
2021 |
Asia |
Iran |
retrospective observational study |
35.10±9.20 |
41 |
10 |
RRMS |
7 |
2 years |
0 |
NM |
32 |
|
|
|
Paybast et al. |
2022 |
Asia |
Iran |
cross-sectional |
37.45 ± 8.768 |
25 |
5 |
CIS:1 |
NM |
NM |
1.77 ± 1.52 |
NM |
1 |
|
|
|
PPMS:1 |
|
||||||||||||||
|
SPMS:4 |
|
||||||||||||||
|
RRMS:19 |
|
||||||||||||||
Discussion
In this meta-analysis, we found that relapse rate after COVID vaccination is substantially lower than after COVID infection which was in line with our assumption of the safety of COVID-19 regarding MS relapse.
Although, several studies demonstrated the effectiveness of COVID-19 in reducing severe illness and death, there is a risk of unexpected side effects due to the way the vaccines interact with the body's immune system. This can lead to inflammatory reactions or worsening of autoimmune diseases like multiple sclerosis shortly after vaccination (24). It is essential to include patients with autoimmune diseases such as MS in clinical trials to ensure that the vaccines are effective and safe for everyone. Without their participation, the vaccines' effectiveness for MS population will remain uncertain, leaving them vulnerable to the virus's severe effects (25). Although, MS patients are anxious about how their condition or their therapies might impact the safety of the COVID-19 vaccines, patients on DMTs are not at a higher risk of experiencing COVID-19 with severe symptoms (26). Multiple sclerosis (MS) patients treated with fingolimod and ocrelizumab may have a reduced immune response, making it important to monitor their SARS-CoV-2 antibody titer after vaccination. This will help preserve the efficacy of the vaccine and ensure that the patients are protected against the virus.
It is more likely that MS patients will suffer from the consequences of the infection, such as acute MS relapse and exacerbation, rather than a severe immune response following vaccination. Therefore, it is crucial for MS patients to take precautions and get vaccinated to protect themselves from the virus (27). Recent studies have suggested that non-live SARS-CoV-2 vaccines may be a safe option for individuals with multiple sclerosis (MS) who are not experiencing an active phase of the disease. Despite research that has disproven any link between vaccination and MS relapses, concerns still persist. Although, MS patients may be hesitant to get vaccinated due to the fear of exacerbating their symptoms, experts suggest these patients to be vaccinated (28).
The COVID-19 pandemic has brought about a global effort to develop vaccines against the virus which have been demonstrated to be effective in preventing acute respiratory distress syndrome (ARDS) and other severe consequences. neurological side effects of SARS-CoV-2 vaccinations have been of concern, especially for those with MS. Most of these side effects are mild and self-limiting, but in some instances, they can be severe enough to require admission to hospital or intensive care unit (ICU). The most common neurological side effect by far is headache followed by cases of Guillain-Barre syndrome (GBS) and venous sinus thrombosis (VST) (29).
Some studies also suggest that post-vaccination demyelination is probably playing a crucial role in relapses and pseudo-relapses of MS patients getting vaccinated (30). The majority of these CNS demyelination cases which are assumed to be vaccine-induced are likely to be a pre-existing or previously unrecognized MS. Autoimmunity after vaccination is a common phenomenon, and two theories that explain this are cross-reactivity and bystander activation. Depending on the type of vaccine, these mechanisms can be more or less relevant. In the case of mRNA vaccines such as Pfizer's COVID-19 vaccine, cross-reactivity may be the cause. This is due to the similarity between the COVID-19 spike protein antibody and myelin basic protein, a protein found in the nervous system that helps insulate nerve fibers. Moreover, the interaction between spike proteins and Angiotensin-Converting Enzyme 2 (ACE2) receptors located in the Blood-Brain Barrier (BBB) and spinal neurons has been reported in several studies. This interaction can lead to bystander activation, where the immune system attacks healthy cells that are not infected with the virus (31).
Achiron et al. conducted a cohort study in 2021 to evaluate the safety of the Pfizer-BioNTech COVID-19 vaccine in MS patients and found that MS patients had similar rates of adverse reactions to what has been reported in the general healthy population following vaccination. No increased risk of relapse activity was observed over a median follow-up of 20 and 38 days after the first and second vaccine doses, respectively. Although, a mild increase in the rate of adverse events has been observed in younger patients and those treated with immunomodulatory drugs, the relapse rate following vaccination was similar compared to the 3-year relapse rate prior to vaccination. Overall, these findings support the safety of COVID-19 vaccination in patients with MS (32) In contrast with these findings a case series presented reactivation cases of MS after administration of COVID vaccine (AstraZeneca and Pfizer-BioNTech). all relapses were clinically and radiologically confirmed and 3 out of 16 presented MS cases have received diagnosis after COVID vaccination (33).
Limitations
An important factor to be considered is the vaccination of MS patients with DMTs because Some DMTs with immunosuppressive effects on vaccine humoral responses, especially S1P modulators and B-cell depleting therapies have the potential to attenuate the post-vaccination adverse auto immune events by controlling the immune system reaction after the vaccine and diminish the rate of CNS inflammation and demyelination. on the other hand, some DMTs decrease the efficacy of COVID-19 vaccines. But the patients often achieve sufficient levels of protective antibodies against COVID-19. (34) . individual circumstances (risk factors, age, MS disease progression and phase, prognosis, and lymphocyte count) should be considered when it comes to optimizing vaccine efficacy. More specific investigations may be issued to recognize the effect of DMT regimen type on post-vaccination MS relapse rate (26).
Formal registries of the type of DMT administered and adjusting the study sample of vaccinated MS patients for their DMT Regimen in the analysis (which unfortunately hasn`t been done in the analyzed studies) and concomitant usage of DMTs that attenuate the autoimmune reactions after vaccination seem to be several helpful steps in protection against vaccine-associated relapses of MS. So, each case needs to be handled analyzed more carefully.
Another important limitation of studying MS relapse rates is the lag between the onset of the initial symptoms and the final diagnosis. This can vary depending on individual health-seeking behavior, healthcare systems, and diagnostic techniques. As a result, post-vaccination relapse rates were found to be higher in younger patients in a recent study with a longer follow-up period. However, studies with short follow-ups may overlook potential associations, while those with too-long follow-ups may dilute or falsely associate triggers with MS relapse. Therefore, it is important to consider the duration of follow-up in MS relapse studies to avoid overlooking or overemphasizing potential associations. So far, studies have confirmed that COVID-19 vaccination is generally well-tolerated in MS patients regardless of the type of vaccine used and should be recommended to all patients regardless of their current DMTs (35).
Conclusion
The advantages of COVID-19 vaccination for MS patients exceed any potential risks. The vaccines produced by Moderna, Pfizer-BioNTech, Oxford-AstraZeneca, and Janssen have been seemed safe for use in MS patients. In fact, MS patients are a priority group for vaccination in the UK. Although, there is no strong link between COVID-19 vaccination and the occurrence or exacerbation of MS, patients experiencing MS exacerbations should wait until their neurological status stabilizes before receiving the vaccine. MS patients should consult with healthcare professionals to determine the best course of action for their needs (36). Taken together, our findings provide an overall safety information in terms of MS relapse for COVID-19 vaccination in patients with MS.
Deceleration
Funding
We do not have any financial support for this study.
Conflict of interest
The authors declare no conflict of interest regarding the publication of this paper.
Availability of data and material
The datasets analyzed during the current study are available upon request with no restriction.
Consent for publication
This manuscript has been approved for publication by all authors.
| 1. Correale J, Gaitán MI, Ysrraelit MC, Fiol MP. Progressive multiple sclerosis: from pathogenic mechanisms to treatment. Brain. 2017;140(3):527-46. https://doi.org/10.1093/brain/aww258 PMid:27794524 |
||||
| 2. Perry VH. The influence of systemic inflammation on inflammation in the brain: implications for chronic neurodegenerative disease. Brain, behavior, and immunity. 2004;18(5):407-13. https://doi.org/10.1016/j.bbi.2004.01.004 PMid:15265532 |
||||
| 3. Perry VH, Holmes C. Microglial priming in neurodegenerative disease. Nature Reviews Neurology. 2014;10(4):217-24. https://doi.org/10.1038/nrneurol.2014.38 PMid:24638131 |
||||
| 4. Najjar S, Najjar A, Chong DJ, Pramanik BK, Kirsch C, Kuzniecky RI, et al. Central nervous system complications associated with SARS-CoV-2 infection: integrative concepts of pathophysiology and case reports. Journal of neuroinflammation. 2020;17(1):1-14. https://doi.org/10.1186/s12974-020-01896-0 PMid:32758257 PMCid:PMC7406702 |
||||
| 5. Wucherpfennig KW. Mechanisms for the induction of autoimmunity by infectious agents. The Journal of clinical investigation. 2001;108(8):1097-104. https://doi.org/10.1172/JCI200114235 PMid:11602615 PMCid:PMC209539 |
||||
| 6. von Herrath MG, Fujinami RS, Whitton JL. Microorganisms and autoimmunity: making the barren field fertile? Nature Reviews Microbiology. 2003;1(2):151-7. https://doi.org/10.1038/nrmicro754 PMid:15035044 |
||||
| 7. Correale J, Fiol M, Gilmore W. The risk of relapses in multiple sclerosis during systemic infections. Neurology. 2006;67(4):652-9. https://doi.org/10.1212/01.wnl.0000233834.09743.3b PMid:16870812 |
||||
| 8. Marrodan M, Alessandro L, Farez MF, Correale J. The role of infections in multiple sclerosis. Multiple Sclerosis Journal. 2019;25(7):891-901. https://doi.org/10.1177/1352458518823940 PMid:30638421 |
||||
| 9. Jakimovski D, Weinstock-Guttman B, Ramanathan M, Dwyer MG, Zivadinov R. Infections, vaccines and autoimmunity: a multiple sclerosis perspective. Vaccines. 2020;8(1):50. https://doi.org/10.3390/vaccines8010050 PMid:32012815 PMCid:PMC7157658 |
||||
| 10. Buljevac D, Flach H, Hop W, Hijdra D, Laman J, Savelkoul H, et al. Prospective study on the relationship between infections and multiple sclerosis exacerbations. Brain. 2002;125(5):952-60. https://doi.org/10.1093/brain/awf098 PMid:11960885 |
||||
| 11. Liu Y, Sawalha AH, Lu Q. COVID-19 and autoimmune diseases. Current opinion in rheumatology. 2021;33(2):155. https://doi.org/10.1097/BOR.0000000000000776 PMid:33332890 PMCid:PMC7880581 |
||||
| 12. Yazdanpanah N, Rezaei N. Autoimmune complications of COVID‐19. Journal of medical virology. 2022;94(1):54-62. https://doi.org/10.1002/jmv.27292 PMid:34427929 PMCid:PMC8661629 |
||||
| 13. Michelena G, Casas M, Eizaguirre MB, Pita MC, Cohen L, Alonso R, et al. ¿ Can COVID-19 exacerbate multiple sclerosis symptoms? A case series analysis. Multiple Sclerosis and Related Disorders. 2022;57:103368. https://doi.org/10.1016/j.msard.2021.103368 PMid:35158474 |
||||
| 14. Barzegar M, Vaheb S, Mirmosayyeb O, Afshari-Safavi A, Nehzat N, Shaygannejad V. Can coronavirus disease 2019 (COVID-19) trigger exacerbation of multiple sclerosis? A retrospective study. Multiple sclerosis and related disorders. 2021;52:102947. https://doi.org/10.1016/j.msard.2021.102947 PMid:33979771 PMCid:PMC8036166 |
||||
| 15. Palao M, Fernández-Díaz E, Gracia-Gil J, Romero-Sánchez CM, Díaz-Maroto I, Segura T. Multiple sclerosis following SARS-CoV-2 infection. Mult Scler Relat Disord. 2020;45:102377. https://doi.org/10.1016/j.msard.2020.102377 PMid:32698095 PMCid:PMC7340057 |
||||
| 16. Etemadifar M, Sedaghat N, Aghababaee A, Kargaran PK, Maracy MR, Ganjalikhani-Hakemi M, et al. COVID-19 and the risk of relapse in multiple sclerosis patients: a fight with no bystander effect? Multiple Sclerosis and Related Disorders. 2021;51:102915. https://doi.org/10.1016/j.msard.2021.102915 PMid:33799284 PMCid:PMC7980521 |
||||
| 17. Huang Y, Rodgers WJ, Middleton RM, Baheerathan A, Tuite-Dalton KA, Ford DV, et al. Willingness to receive a COVID-19 vaccine in people with multiple sclerosis-UK MS Register survey. Multiple sclerosis and related disorders. 2021;55:103175. https://doi.org/10.1016/j.msard.2021.103175 PMid:34343866 PMCid:PMC8313796 |
||||
| 18. Ascherio A, Zhang SM, Hernán MA, Olek MJ, Coplan PM, Brodovicz K, et al. Hepatitis B vaccination and the risk of multiple sclerosis. New England Journal of Medicine. 2001;344(5):327-32. https://doi.org/10.1056/NEJM200102013440502 PMid:11172163 |
||||
| 19. Toplak N, Kveder T, Trampuš-Bakija A, Šubelj V, Čučnik S, Avčin T. Autoimmune response following annual influenza vaccination in 92 apparently healthy adults. Autoimmunity reviews. 2008;8(2):134-8. https://doi.org/10.1016/j.autrev.2008.07.008 PMid:18700173 |
||||
| 20. Ehde DM, Roberts MK, Humbert AT, Herring TE, Alschuler KN. COVID-19 vaccine hesitancy in adults with multiple sclerosis in the United States: A follow up survey during the initial vaccine rollout in 2021. Multiple sclerosis and related disorders. 2021;54:103163. https://doi.org/10.1016/j.msard.2021.103163 PMid:34325399 PMCid:PMC8295053 |
||||
| 21. Nistri R, Barbuti E, Rinaldi V, Tufano L, Pozzilli V, Ianniello A, et al. Case report: multiple sclerosis relapses after vaccination against SARS-CoV2: a series of clinical cases. Frontiers in neurology. 2021:1866. https://doi.org/10.3389/fneur.2021.765954 PMid:34744992 PMCid:PMC8569136 |
||||
| 22. Fragoso YD, Gomes S, Gonçalves MVM, Junior EM, de Oliveira BES, Rocha CF, et al. New relapse of multiple sclerosis and neuromyelitis optica as a potential adverse event of AstraZeneca AZD1222 vaccination for COVID-19. Multiple Sclerosis and Related Disorders. 2022;57:103321. https://doi.org/10.1016/j.msard.2021.103321 PMid:35158439 PMCid:PMC8511887 |
||||
| 23. Moher D, Liberati A, Tetzlaff J, Altman DG, The PG. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLOS Medicine. 2009;6(7):e1000097. https://doi.org/10.1371/journal.pmed.1000097 PMid:19621072 PMCid:PMC2707599 |
||||
| 24. Doubrovinskaia S, Mooshage CM, Seliger C, Lorenz H-M, Nagel S, Lehnert P, et al. Neurological autoimmune diseases following vaccinations against severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2): A follow-up study. European Journal of Neurology. 2023;30(2):463-73. https://doi.org/10.1111/ene.15602 PMid:36259114 PMCid:PMC9874608 |
||||
| 25. Monschein T, Hartung HP, Zrzavy T, Barnett M, Boxberger N, Berger T, et al. Vaccination and multiple sclerosis in the era of the COVID-19 pandemic. J Neurol Neurosurg Psychiatry. 2021;92(10):1033-43. https://doi.org/10.1136/jnnp-2021-326839 PMid:34353858 PMCid:PMC8458056 |
||||
| 26. Pernicová E, Macounová P, Krsek M, Maďar R. Summary of safety and efficacy of COVID-19 vaccination in patients with multiple sclerosis. European Neurology. 2023:1-. https://doi.org/10.1159/000529982 PMid:36871554 PMCid:PMC10614228 |
||||
| 27. Witman Tsur S, Adrian Zaher E, Tsur M, Kania K, Kalinowska-Łyszczarz A. Current Immunological and Clinical Perspective on Vaccinations in Multiple Sclerosis Patients: Are They Safe after All? Int J Mol Sci. 2021;22(8). https://doi.org/10.3390/ijms22083859 PMid:33917860 PMCid:PMC8068297 |
||||
| 28. Ciotti JR, Perantie DC, Moss BP, Fitzgerald KC, Cohen JA, Mowry EM, et al. Perspectives and experiences with COVID-19 vaccines in people with MS. Mult Scler J Exp Transl Clin. 2022;8(1):20552173221085242. https://doi.org/10.1177/20552173221085242 PMid:35273809 PMCid:PMC8902317 |
||||
| 29. Finsterer J. Neurological side effects of SARS-CoV-2 vaccinations. Acta Neurologica Scandinavica. 2022;145(1):5-9. https://doi.org/10.1111/ane.13550 PMid:34750810 PMCid:PMC8653194 |
||||
| 30. Lu L, Xiong W, Mu J, Zhang Q, Zhang H, Zou L, et al. The potential neurological effect of the COVID-19 vaccines: A review. Acta Neurologica Scandinavica. 2021;144(1):3-12. https://doi.org/10.1111/ane.13417 PMid:33779985 PMCid:PMC8250748 |
||||
| 31. Farez MF, Correale J, Armstrong MJ, Rae-Grant A, Gloss D, Donley D, et al. Practice guideline update summary: Vaccine-preventable infections and immunization in multiple sclerosis: Report of the Guideline Development, Dissemination, and Implementation Subcommittee of the American Academy of Neurology. Neurology. 2019;93(13):584-94. https://doi.org/10.1212/WNL.0000000000008157 PMid:31462584 |
||||
| 32. Achiron A, Dolev M, Menascu S, Zohar D-N, Dreyer-Alster S, Miron S, et al. COVID-19 vaccination in patients with multiple sclerosis: What we have learnt by February 2021. Multiple Sclerosis Journal. 2021;27(6):864-70. https://doi.org/10.1177/13524585211003476 PMid:33856242 PMCid:PMC8114441 |
||||
| 33. Nistri R, Barbuti E, Rinaldi V, Tufano L, Pozzilli V, Ianniello A, et al. Case Report: Multiple Sclerosis Relapses After Vaccination Against SARS-CoV2: A Series of Clinical Cases. Frontiers in Neurology. 2021;12. https://doi.org/10.3389/fneur.2021.765954 PMid:34744992 PMCid:PMC8569136 |
||||
| 34. Witman Tsur S, Adrian Zaher E, Tsur M, Kania K, Kalinowska-Łyszczarz A. Current Immunological and Clinical Perspective on Vaccinations in Multiple Sclerosis Patients: Are They Safe after All? International Journal of Molecular Sciences [Internet]. 2021; 22(8). https://doi.org/10.3390/ijms22083859 PMid:33917860 PMCid:PMC8068297 |
||||
| 35. Diem L, Friedli C, Chan A, Salmen A, Hoepner R. Vaccine Hesitancy in Patients With Multiple Sclerosis: Preparing for the SARS-CoV-2 Vaccination Challenge. Neurol Neuroimmunol Neuroinflamm. 2021;8(3). https://doi.org/10.1212/NXI.0000000000000991 PMid:33811158 PMCid:PMC8018793 |
||||
| 36. Boyko AN, Sivertseva SA, Chemakina DS, Spirin NN, Bykova OV, Guseva ME. Vaccination and Multiple Sclerosis - Current Situation. Neuroscience and Behavioral Physiology. 2022;52(4):486-90. https://doi.org/10.1007/s11055-022-01265-9 PMid:35875700 PMCid:PMC9296221 |
||||
| Article View | 796 |
| PDF Download | 461 |