Document Type : Original Communication
Keywords
Subjects
Background
Brain malformations are among the most common fetal malformations (1) and are among the main causes of pregnancy termination (2). Based on the population studied the prevalence of brain anomalies varies from 1.07% in Japan to 4.3% in Taiwan (3), with global prevalence roughly reaching 1 per 100 pregnancies (4). Brain anomalies are classified into two main groups acquired and developmental brain anomalies, each with its causes (5, 6). Developmental anomalies occur on a genetic deficit background and thus heralds an increased risk of re-occurrence in future pregnancies. Given that fetal brain malformations have a wide range of negative consequences for parents, including but not limited to their financial status, quality of life, and, most importantly, psychological well-being, timely and accurate diagnosis appears critical both for planning next steps in the affected pregnancy and counseling future pregnancies (7, 8).
The well-timed and accurate diagnosis of fetal abnormalities can immensely improve the care given to the parents and help to save a considerable budget for governments around the world (9). For decades, prenatal US has been continually considered the preferred method of assessing fetal brain morphology, as it offers a real-time examination, is non-invasive and easy to operate, is reproducible, inexpensive, and provides a high diagnostic yield at an appropriate precision (10). Despite all of the mentioned advantages, ultrasound imaging is operator dependent and of limited value in maternal obesity, adverse fetal position, and multiple pregnancies, and also generates images with relatively low contrast resolution of soft tissues (11). Additionally, acoustic shadows from the fetal calvarium (especially in later pregnancies) confer imaging artifacts that suppress the quality of images, sometimes to such an extent that even gross anatomic features cannot be visualized (12). Lately, prenatal NSG has been widely implemented for diagnosing brain abnormalities during pregnancy (13). In most studies, MRI and NSG have been reported to be equally effective and superior to the US exam for diagnosing fetal brain anomalies (14). In a recent study conducted by the ENSO group, among fetuses diagnosed with isolated corpus callosum anomaly in antenatal NSG, MRI could identify additional anomalies in 11.2%, which were mainly abnormalities of the cortex development (15). Moreover, in another study, the ENSO Working Group found that in fetuses with isolated mild to moderate ventriculomegaly in multiplanar NSG, fetal MRI detects associated CNS anomalies in 5.4% of cases (16). Contradictory findings in the literature may be due to factors such as small sample sizes in relevant studies or different fetal ages at the time of the NSG exam (17). To overcome ultrasound limitations, some previous studies have proposed MRI as a valuable complementary modality of fetal brain evaluation in conjunction with US and NSG imaging for prenatal brain assessment (4, 5). In a recent meta-analysis, standard US was concluded to be an adequate screening tool in antenatal assessments, although MRI was recommended for those with abnormal brains on US as it may add diagnostic information in nearly 22.2% of cases (18). MRI depicts morphological features of the developing fetal brain in detail and at great spatial and contrast resolution, visualizing early and subtle structural deficits with acceptable accuracy (11, 19). Besides, MRI delineates the cerebral and cerebellar cortex and achieves a satisfactory visualization of subarachnoid space as MR images are not disturbed by the calvarium (20).
Continuous advancements in the imaging unit hardware and image processing software industries necessitate a continuous increase in the knowledge and level of experience of sonographers and radiologists to use this equipment optimally and to the best of their abilities, even though familiarity with US, NSG, and MRI for evaluating fetal brain is increasing incrementally (21). This study aims to compare the utility of MRI, US, and NSG for diagnosing fetal brain anomalies.
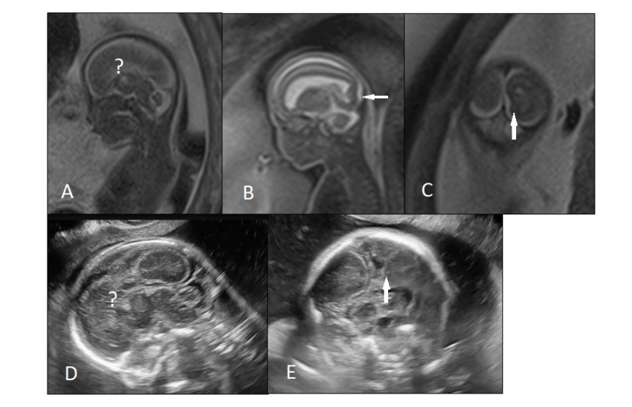
Figure 1. An 18 weeks fetus with mild ventriculomegaly and suspected corpus callosum abnormality was referred for fetal MRI. A, B, C) T2-weighted MRI images showed complete agenesis of corpus callosum and unilateral abnormal sulcation(arrow) in occipital horn. D, E) Transvaginal neurosonography found similar findings.
Methods
Design and setting
This prospective, observational, single-center study was conducted on pregnant women who were referred to our tertiary referral university hospital between 2017 and 2021. This study was approved by the institutional ethics committee and was conducted adhering to the Declaration of Helsinki. Informed written consent was obtained from all patients.
Patients and data acquisition
Participating women had a history of previous pregnancies with CNS anomalies or were pregnant with fetuses suspected of having brain abnormalities on a recent screening ultrasound exam. Investigated fetuses underwent karyotyping and were tested for TORCH infections. All study subjects underwent MRI one to two weeks after the ultrasound exam, and transvaginal NSG was undertaken within one week after MRI for all of the investigated fetuses. Based on the US-MRI concordancy, subjects were divided into four subgroups: (a) the MRI/NSG findings confirmed the US findings; (b) the MRI/NSG findings supplemented the US findings (Figure 1); (c) the MRI/NSG findings contradicted the initial US impression; and (d) the MRI/NSG findings ruled out the initial US diagnosis (false positive US).
In subgroup a, US, NSG, and MRI findings were concordant; however, in subgroups b-d, MRI/NSG findings were discordant with US findings. Cases of MRI-NSG discordance were also outlined in the same manner and were subdivided into two groups: (1) concordance between NSG and MRI; (2) and NSG-MRI discordance (Figure 2).
Neurosonography (NSG)
|
Table 1. Demographic and clinical characteristics of subjects.
*Mean ± SD **N (%) aOf 36 fetuses who were karyotyped, all returned normal results. |
||||||||||||||||||||||||||||||||||||
All of the investigated fetuses underwent an NSG exam. NSG exams were performed by a 7 to 10 MHz multifrequency transducer (via transvaginal probing), or convex 3-5 MHz transducer (transabdominal approach) when the fetus position was suboptimal for the transvaginal exam, using an affinity 70 G ultrasound machine (Philips, Amsterdam, Netherlands). A perinatologist skilled at fetal NSG, with more than 10 years of experience, performed and interpreted NSG exams.
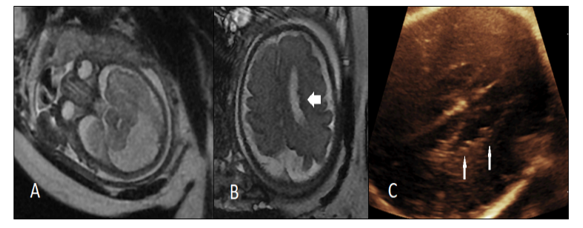
Figure 2. A 34 weeks fetus with megacisternamagna was referred for fetal MRI. A, B) T2-weighted MRI showed megacisternamagna and unilateral periventricular heterotopia (arrow). C) Neurosonography at the same day of MRI found similar periventricular heterotopia (arrows).
Prenatal brain MRI
MR images were taken at 1.5T (GE Healthcare, discovery 750 GEM), including the T1W, T2W, and DWI sequences over nearly 30 minutes for each case. Following MRI sequences were included at a slice thickness of 4 mm: (a) steady-state T1-weighted imaging in the axial plan; (b) single-shot fast spin-echo T2-weighted imaging in three orthogonal plans; (c) fast multiplane sequences spoiled gradient-recalled acquisition in the axial plane; and (d) diffusion-weighted imaging (DWI) using echo planar imaging (EPI) in the axial plane without breath holding and at b-values of 0 and 800 s/mm2. For SSFSE images, MR parameters were set at TR/TE: 6000/70 ms, a field of view: 320400 mm, matrix: 128*128, slice thickness/spacing: 4.00/1.00 mm, bandwidth: 250 kHz, with an acquisition time of 20 s for each case. Two radiologists with 8 and 24 years of experience in obstetric ultrasonography performed and interpreted the encoded MR images and resolved discrepancies by consensus.
|
Table 2. Case-based brain US, NSG and MRI concordance.
US; standard ultrasound imaging; NSG, neurosonography. |
||||||||||||||||||||||||||||||||||||
Perinatal/Postnatal follow-up
Live births were followed for 18 months to assess the course of postnatal neurodevelopment, although some of the fetuses (especially those who did not show concordancy between any of the imaging modalities) did not comply with the follow-up schedule and were followed for 2-17 months postnatally. Follow-up appointments were set at 1-month intervals. In follow-up assessments, infants went through a comprehensive neurological examination by an experienced neuro pediatrician. Some of the fetuses also underwent postnatal MRI.
Statistical analysis
Raw data was fed into SPSS v. 22.0 (IBM Inc., Chicago, Ill., USA). Qualitative variables were reported as frequency and percentage, and quantitative variables were represented by their mean and standard deviation. A chi-square test was employed to evaluate the association between perinatal and postnatal outcomes and the concordancy between findings from various imaging modalities. The statistical significance level was set at p <0.05.
Table 3. Describe MRI and NS findings with additional findings on MRI.
|
Patient |
NSG findings |
Additional finding in MRI |
Time of MRI (week) |
F/U |
Time of F/U (month) |
|
1 |
Severe VM, PMG |
Brain atrophy, periventricular heterotopia |
35 |
Live birth with abnormal evolution |
5 |
|
2 |
Normal |
Mild unilateral IVH |
22 |
Live birth with normal evolution |
10 |
|
3 |
Microcephaly brain atrophy, mild perisylvian PMG |
Extensive perisylvian PMG |
30 |
Live birth with abnormal evolution |
4 |
|
4 |
Moderate VM |
IVH |
24 |
Termination |
- |
|
5 |
moderate VM, Chiari2, Myelomeningocele |
Unilateral IVH |
17 |
Termination |
- |
|
6 |
Hemivertebrae |
IVH |
22 |
Live birth with normal evolution |
2 |
|
7 |
Chiari-2 malformation |
Sacral myelocele, tethered cord |
19 |
Termination |
- |
|
8 |
Mild VM |
Bilateral GMH |
31 |
Live birth with normal evolution |
3 |
|
9 |
Apert syndrome, mild VM |
Acrocephaly, temporal PMG |
20 |
Termination |
- |
|
10 |
Normal |
Unilateral GMH |
25 |
Live birth with normal evolution |
5 |
|
11 |
Normal |
Unilateral IVH |
25 |
Termination |
- |
|
12 |
Mild VM |
IVH |
36 |
Termination |
- |
|
13 |
Unilateral mild VM |
Unilateral GMH |
22 |
Live birth with normal evolution |
4 |
|
14 |
Microcephaly, Perisylvian PMG, cerebellum dysplasia |
Periventricular cyst |
32 |
Intrauterine death |
- |
|
15 |
Normal |
Unilateral mild IVH |
23 |
Termination |
- |
|
16 |
Normal |
Bilateral GMH |
23 |
Live birth with normal evolution |
9 |
|
17 |
Mild unilateral IVH |
Bilateral IVH |
23 |
Live birth with normal evolution |
2 |
|
18 |
Moderate unilateral VM, mega cisterna magna, CC dysgenesis
|
Periventricular heterotopia |
35 |
Live birth with normal evolution |
4 |
|
19 |
Severe bilateral VM, periventricular heterotopia |
IVH and IPH (grade4), porencephalic cyst |
34 |
Live birth with normal evolution |
3 |
|
20 |
Cerebellum hypoplasia, VM, vein of Galen aneurysm, cerebellar AVM |
Brain edema |
35 |
Death after birth |
- |
|
21 |
Mild unilateral VM |
Periventricular heterotopia |
32 |
Live birth with normal evolution |
8 |
|
22 |
Mild unilateral VM, Mega cisterna magna, cerebellum hypoplasia |
Bilateral IVH |
33 |
Death after birth |
- |
|
23 |
Severe bilateral VM, CC dysgenesis, (HIE) |
PMG |
37 |
Live birth with normal evolution |
17 |
|
24 |
Mild microcephaly, cerebellum hypoplasia, CC dysgenesis |
Periventricular heterotopia |
22 |
Termination |
- |
|
25 |
Interhemispheric cyst |
CC dysgenesis |
33 |
Live birth with normal evolution |
7 |
|
26 |
Mild unilateral VM, PMG |
Periventricular heterotopia |
21 |
Termination |
- |
|
27 |
Normal |
Bilateral IVH, brain infarct |
23 |
Intrauterine death |
- |
|
28 |
Moderate VM, PMG, cephalocele, abnormal cerebellar vermis, Wallenberg Syndrome |
Periventricular heterotopia |
25 |
Intrauterine death |
- |
|
29 |
Mild VM, IVH |
Brain infarct |
21 |
Termination |
|
|
30 |
Normal |
Mild unilateral IVH |
20 |
Live birth with normal evolution |
14 |
|
31 |
Normal |
Unilateral GMH |
22 |
Live birth with normal evolution |
2 |
|
32 |
Hemivertebrae, tethered cord, diastematomyelia, closed spina bifida |
Syrinx |
28 |
Live birth with normal evolution |
6 |
AVM, arteriovenous malformation; CC, corpus callosum; DWI, diffusion weighted imaging; GMH, germinal matrix hemorrhage; F/U, follow-up; IPH, intraparenchymal hemorrhage; IVH, intraventricular hemorrhage; NSG, neurosonography; PMG, polymicrogyria; VM, ventriculomegaly.
Results
140 pregnant women with a mean maternal age of 30.88±5.61 years were enrolled. Nearly one-third (29.6%) of mothers were engaged in consanguineous marriages, and 4.3% reported a previous pregnancy history of fetal CNS anomalies. Fetuses were studied at a mean gestational age of 28.09±4.95 weeks. Of all the fetuses investigated, 36.3% were female, 25.4% had been karyotyped (all returned normal results), and 2.8% had normal brain MRI (Table 1).
Brain US, NSG, and MRI findings showed a significantly high level of concordance. Most common CNS pathologies found in all imaging modalities concordantly were ventriculomegaly (48.6%), intracranial hemorrhages (12.9%), corpus callosum anomalies (11.4%), and cortical malformation (13.5%). As Table 2 shows, among cases whose brain US was discordant with NSG/MRI, 73.2% had additional findings in NSG/MRI (Figure 1), 23.9% were diagnosed with other brain anomalies, and 2.8% showed a normal brain in NSG/MRI (false positive US). The US exams performed after the 20th week of pregnancy showed a significantly higher concordancy with NSG/MRI, and diagnosed brain abnormalities with a higher accuracy (Figure 3). Generally, 54.9% of cases whose brain US was discordant with NSG/MRI showed similar findings in NSG and MRI (Table 2).
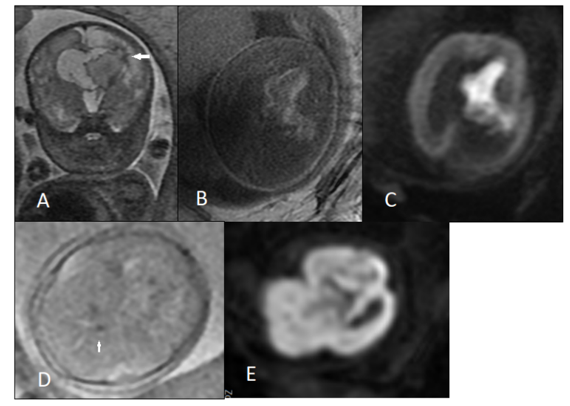
Figure 3. A 30 weeks fetus with severe ventriculomegaly and IVH was referred for fetal MRI. A, B, C) T2-weighted, T1-weighted and DWI images (respectively) showed unilateral severe ventriculomegaly y, periventricular edema and acute IVH. In fig A, focal extension of hemorrhage to adjacent parenchyma (arrow) is evident (IVH grade 4). But this parenchymal extension was not detected by neurosongraphy. D, E) Another 23 weeks fetus with recent radiofrequency ablation of co-twin showed germinal matrix hemorrhage (arrow) and whole brain infarct in DWI (E) with normal neurosonography.
Among all enrolled cases, NSG-MRI discordance was found in 22.9% (32) of fetuses, all showing additional findings in MRI, while none showed additional or contradicting findings on NSG (Figure 2). Table 3 describes the NSG findings in each of these 32 cases and shows any additional MRI features that were not visible on NSG. Interestingly, 4 fetuses had normal brains in NSG exams but were diagnosed with IVH/GMH in MRI. MRI was superior to NSG to detect intracranial hemorrhage and cortical malformations and offered a more accurate estimation of the extension of cortical malformation. Table 3 also outlines the final delivery outcome and duration of follow-up for each of these cases.
In Table 4, perinatal and postnatal outcomes are presented. In 2 cases, who were suspected to have craniosynostosis, black pouch cyst, and vermin hypoplasia in the US, MRI/NSG ruled out the initial US diagnosis.
In Table 5, perinatal and postnatal outcomes are stratified based on the concordance of the findings shown in different imaging modalities. As demonstrated in Table 5, live births with successful postnatal normal neurodevelopment were more likely to show concordancy between US, NSG, and MRI. Live births with abnormal postnatal neurodevelopment and fetuses who were demised before delivery more frequently showed discordancy between various imaging modalities, while the difference remained non-significant in either subgroup (p = 0.08).
From another perspective, normal brain imaging was reported with higher repeatability in various imaging modalities and could significantly predict normal postnatal neurodevelopment (P value 0.0001).
Among 140 pregnancies, 6 resulted in intrauterine fetal demise, and 17 pregnancies were terminated. Of 117 live births, 11 died after birth, 10 showed abnormal neurodevelopment, and 96 showed normal neurodevelopment postnatally.
Discussion
One of the most challenging yet prevalent fetal conditions that obstetricians and parents might face during pregnancy and post-delivery is CNS anomalies (22). It is critical to detect these anomalies antenatally to advise parents on whether they can afford the resources required to raise and support their children (23). US exam is a non-invasive, non-radiating, and effective modality of diagnosis capable of detecting CNS anomalies to an acceptable level. Nevertheless, the nonspecific appearance of some CNS anomalies in the US, operator dependency, and some technical factors may limit its utility in some cases and necessitate further imaging assessment (17). Fetal MRI as a complementary imaging tool would assist in diagnosis to a great extent when brain US results are equivocal or need confirmation, especially in suspected cases of delicate morphological abnormalities (24) While not being very operator-dependent, performing MRI is safe in pregnancy and requires minimal technical effort while providing images with high contrast and spatial resolution.
|
Table 4. The patients’ follow up results.
|
||||||||||||||||||||||||||||||||
The present study found that US is concordant with NSG and MRI in 49.3% of cases, and in the remaining 50.7%, fetal MRI provides additional findings in approximately 73.2% of antenatal US, which may sometimes change the diagnosis or even reveal a false positive diagnosis by US. This finding is in keeping with the results of an investigation conducted by Levine et al., who reported that nearly 40% of fetuses demonstrate MRI findings that change the US diagnosis and suggest other CNS anomalies (25). Sonigo et al. studied approximately 400 fetuses with brain abnormalities and concluded that MRI could be used as a complementary method of fetal brain imaging alongside the US to achieve a higher diagnostic yield and come up with a more accurate diagnosis early enough to prepare the parents and care system for optimal pregnancy and postnatal care (26). Van Der Knoop et al. concluded that multiplanar NSG detects periventricular echogenicity changes, IVH, and/or changes in basal ganglia or thalami with a higher sensitivity compared to the standard axial ultrasound planes (27).
According to our findings, in 22.9% of study subjects, MRI unraveled additional findings, which were not seen on NSG. These results are in keeping with the results of a study by the ENSO Working Group, which compared the detection rate of CNS anomalies in NSG and MRI, and reported that MRI detects additional intracranial hemorrhage, polymicrogyria, and lissencephaly in 26.7%, 20%, and 13.3% of cases (16). Likewise, in our study, the majority of CNS anomalies that were found in MRI and missed in NSG were intracranial hemorrhage, polymicrogyria, and grey matter heterotopia. They also reported that MRI detects additional corpus callosum anomalies (agenesis or dysgenesis) than NSG in only 3.3%-6.7% of cases, which is by our study that reported no case of corpus callosum anomalies additionally found in MRI. However, Van Der Knoop et al. did not confirm the added diagnostic value of MRI when performed after NSG (27). Additionally, Malinger et al. found that dedicated NSG is equally accurate to MRI for diagnosing fetal brain anomalies. In their study, MRI confirmed the NSG diagnosis for the majority of the cases; however, in some cases MRI-NSG discordancy was noted, either of them supplementing the other modality or suggesting a different diagnosis (14).
As per our result, findings from US, NSG, and MRI were concordant in nearly half of the cases, and in the majority of cases with discordant imaging findings, MRI added to the diagnostic yield. Malinger et al. (14), however, found that different imaging modalities are not significantly concordant. Numerous factors may lead to these controversial results, including imaging protocol and interpretation guidelines that might explain systematic errors, the expertise of the staff involved with taking and interpreting images that might explain individual errors, and the gestational age at which imaging is done. A previous study found that performing US after the 20th week of gestation enhances its diagnostic accuracy for detecting CNS anomalies (28). Our results demonstrated that the discrepancy between the findings from different imaging methods would be lower after the 20th week of pregnancy, and standard fetal US performed after 20 weeks of gestation diagnose brain abnormalities with a higher sensitivity and accuracy. However, the ENSO Working Group concluded that performing fetal brain imaging after 24 weeks of gestation remarkably enhances the detection rate for CNS anomalies (16). Moreover, Malinger et al. reported that performing US before the 25th week of pregnancy can lead to an incorrect diagnosis. Given the wide range of reported optimal gestational age for performing fetal imaging, to obtain the most detailed images from CNS and achieve the most accurate diagnosis further large-scale studies are needed to reach a reasonable and valid consensus.
Our study is subjected to some limitations. First and foremost, the limited number of enrolled cases will cause sampling bias, and further populous investigations are needed for more confident results. Second, genetic tests were not performed for the majority of study subjects, and some known predisposing genetic factors might have remained undetected. Although genetic assessments, such as microarray or whole genome analyses, are not daily routine practices and might not be available in some centers, testing the concordancy of different imaging modalities for detecting CNS anomalies in particular genetic diseases would be of clinical advantage. Relatively short-term postnatal follow-up may not be able to outline an accurate assessment of neuro-developmental that continues to early childhood. Longer-term studies may mark out some of the cases which are initially showing normal neurodevelopment but experience delayed or disturbed development afterward. Finally, some of the fetuses with mild CNS abnormalities (e.g., mild ventriculomegaly) or those who were asymptomatic postnatally did not undergo postnatal MR and some others did not comply with pre-scheduled follow-up appointments.
Conclusions
Fetal MRI and prenatal NSG are more accurate for diagnosing CNS anomalies than routine prenatal US assessments. Prenatal MRI is the most accurate imaging modality of assessment for detecting CNS anomalies antenatally, and might supplement the US/NSG findings, and sometimes contradicts or excludes the initial US diagnosis. In fetuses with CNS anomalies in NSG, MRI might add clinically relevant information in almost 23% of the cases. The diagnostic yield of prenatal MRI might be even higher if the pregnancy outcome is dismal, although in our study the difference was not significant and this needs to be further investigated by larger-scale studies.
Abbreviations
VAS: Magnetic resonance imaging, US: ultrasound, NSG: neurosonography, CNS: central nervous system, TORCH: toxoplasmosis, rubella cytomegalovirus, herpes simplex, and HIV IVH: Intraventricular hemorrhage, GMH: Germinal matrix hemorrhage.
Statements and Declarations
Ethics approval
The proposal of this plan with the code IR.TUMS.IKHC.REC has been approved by the ethics committee of Tehran University of Medical Sciences.
Patient consent statement
Written informed consent was obtained from the patient to publish this report in accordance with the journal's patient consent policy.
Data availability statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Funding
No fund has been received regarding this study.
Conflict of interests
The all authors declare that there is no the conflict of interest regarding the publication of this article.
Authors' contributions
FZ designed study, and wrote primary draft. BM & HH supervised the study and helped for designing study and collecting the data, MSH & SH & MHG advised study and helped for collecting the data. JA helped for analyzed of data, MAK helped for design study and analyzed of data and MSH wrote primary draft and Submission. MHG edited the final draft and submitted the manuscript.
Acknowledgements
Our thanks go out to all the parents who participated in the study.
| 1. Goergen SK, Alibrahim E, Govender N, Stanislavsky A, Abel C, Prystupa S, et al. Diagnostic assessment of foetal brain malformations with intra-uterine MRI versus perinatal post-mortem MRI. Neuroradiology. 2019;61(8):921-34. https://doi.org/10.1007/s00234-019-02218-9 PMid:31076826 PMCid:PMC6620257 |
||||
| 2. Vaknin Z, Lahat Y, Barel O, Ben-Ami I, Reish O, Herman A, et al. Termination of pregnancy due to fetal abnormalities performed after 23 weeks' gestation: analysis of indications in 144 cases from a single medical center. Fetal diagnosis and therapy. 2009;25(2):291-6. https://doi.org/10.1159/000229501 PMid:19628945 |
||||
| 3. Hamisa M, Dabees N, Ataalla WM, Ziada DH. Magnetic resonance imaging versus Ultrasound examination in detection of prenatal fetal brain anomalies. The Egyptian Journal of Radiology and Nuclear Medicine. 2013;44(3):665-72. https://doi.org/10.1016/j.ejrnm.2013.05.004 |
||||
| 4. Frick N, Fazelnia C, Kanzian K, Hitzl W, Fischer T, Forstner R, et al. The reliability of fetal MRI in the assessment of brain malformations. Fetal diagnosis and therapy. 2015;37(2):93-101. https://doi.org/10.1159/000363652 PMid:25138047 |
||||
| 5. Girard N, Chaumoitre K, Chapon F, Pineau S, Barberet M, Brunel H, editors. Fetal magnetic resonance imaging of acquired and developmental brain anomalies. Seminars in perinatology; 2009: Elsevier. https://doi.org/10.1053/j.semperi.2009.04.007 PMid:19631084 |
||||
| 6. Glinianaia SV, Tennant PW, Rankin J. Risk estimates of recurrent congenital anomalies in the UK: a population-based register study. BMC medicine. 2017;15(1):1-14. https://doi.org/10.1186/s12916-017-0789-5 PMid:28137281 PMCid:PMC5282823 |
||||
| 7. Mohammed AR, Mohammed S, AbdulFatah A. Congenital anomalies among children: knowledge and attitude of Egyptian and Saudi mothers. Biol Agr Healthcare. 2013;3:2224-3208. | ||||
| 8. Joel-Medewase V, Adeleye A. The social-economic and family background of the child with a CNS birth defect in a developing country in the current era. Nigerian Journal of Paediatrics. 2015;42(1):55-8. https://doi.org/10.4314/njp.v42i1.12 |
||||
| 9. Gonçalves L, Lee W, Mody S, Shetty A, Sangi‐Haghpeykar H, Romero R. Diagnostic accuracy of ultrasonography and magnetic resonance imaging for the detection of fetal anomalies: a blinded case-control study. Ultrasound in Obstetrics & Gynecology. 2016;48(2):185-92. https://doi.org/10.1002/uog.15774 PMid:26444861 PMCid:PMC5987216 |
||||
| 10. Rossi A, Prefumo F. Additional value of fetal magnetic resonance imaging in the prenatal diagnosis of central nervous system anomalies: a systematic review of the literature. Ultrasound in Obstetrics & Gynecology. 2014;44(4):388-93. https://doi.org/10.1002/uog.13429 PMid:24890732 |
||||
| 11. Moradi B, Shirazi M, Alibeigi Nezhad Z, Seyed Saadat N, Hashemi H, Kazemi MA, et al. Differences in the Brain Cortical Thickness and Area of Different Lobes Between Fetuses with Intrauterine Growth Restriction and Controls Based on 3-Tesla Magnetic Resonance Imaging (MRI). Iranian Journal of Radiology. 2021;18(2). https://doi.org/10.5812/iranjradiol.106888 |
||||
| 12. Zhou Q, Liang J, Wang N, Zha Q, Yan R, Li R, et al. The characteristics of fetal central nervous system abnormalities in prenatal magnetic resonance imaging and ultrasonography and their relationship with chromosomal disorders. INTERNATIONAL JOURNAL OF CLINICAL AND EXPERIMENTAL MEDICINE. 2019;12(4):4076-87. | ||||
| 13. Benacerraf BR, Shipp TD, Bromley B, Levine D. What does magnetic resonance imaging add to the prenatal sonographic diagnosis of ventriculomegaly? Journal of ultrasound in medicine. 2007;26(11):1513-22. https://doi.org/10.7863/jum.2007.26.11.1513 PMid:17957045 PMCid:PMC2262180 |
||||
| 14. Malinger G, Ben‐Sira L, Lev D, Ben‐Aroya Z, Kidron D, Lerman‐Sagie T. Fetal brain imaging: a comparison between magnetic resonance imaging and dedicated neurosonography. Ultrasound in Obstetrics and Gynecology: The Official Journal of the International Society of Ultrasound in Obstetrics and Gynecology. 2004;23(4):333-40. https://doi.org/10.1002/uog.1016 PMid:15065181 |
||||
| 15. D'Antonio F, Sileo FG, group ENw, Sileo FG, Pilu G, Prayer D, et al. Role of prenatal magnetic resonance imaging in fetuses with isolated anomalies of the corpus callosum: a multinational study. Ultrasound in Obstetrics & Gynecology. 2021. | ||||
| 16. Group EW, Di Mascio D, Khalil A, Thilaganathan B, Rizzo G, Buca D, et al. Role of prenatal magnetic resonance imaging in fetuses with isolated mild or moderate ventriculomegaly in the era of neurosonography: international multicenter study. Ultrasound in Obstetrics & Gynecology. 2020;56(3):340-7. https://doi.org/10.1002/uog.21974 PMid:31917496 |
||||
| 17. Moradi B, Naybandi Atashi S, Kazemi M, Rahmani M. Fetal intraventricular hemorrhage: does advanced neurosonography work better than magnetic resonance imaging? Ultrasound in Obstetrics & Gynecology. 2021;57(3):507-. https://doi.org/10.1002/uog.23580 PMid:33646638 |
||||
| 18. Moradi B, Kazemi MA, Hashemi H, Miratashi Yazdi SN. Fetal brain imaging: A comparison between fetal ultrasonography and intra uterine magnetic resonance imaging (a systematic review and meta-analysis). Journal of clinical ultrasound. In press. https://doi.org/10.1002/jcu.23158. https://doi.org/10.1002/jcu.23158 PMid:35266167 |
||||
| 19. Fogliarini C, Chaumoitre K, Chapon F, Fernandez C, Lévrier O, Figarella-Branger D, et al. Assessment of cortical maturation with prenatal MRI. Part I: normal cortical maturation. European radiology. 2005;15(8):1671-85. https://doi.org/10.1007/s00330-005-2782-1 PMid:15856237 |
||||
| 20. Girard N, Chaumoitre K, Confort-Gouny S, Viola A, Levrier O. Magnetic resonance imaging and the detection of fetal brain anomalies, injury, and physiologic adaptations. Current Opinion in Obstetrics and Gynecology. 2006;18(2):164-76. https://doi.org/10.1097/01.gco.0000193002.58158.07 PMid:16601478 |
||||
| 21. Blondiaux E, Garel C. Fetal cerebral imaging-ultrasound vs. MRI: an update. Acta Radiologica. 2013;54(9):1046-54. https://doi.org/10.1258/ar.2012.120428 PMid:23012483 |
||||
| 22. Levine D, Barnes PD, Madsen JR, Li W, Edelman RR. Fetal central nervous system anomalies: MR imaging augments sonographic diagnosis. Radiology. 1997;204(3):635-42. https://doi.org/10.1148/radiology.204.3.9280237 PMid:9280237 |
||||
| 23. Hart AR, Embleton ND, Bradburn M, Connolly DJ, Mandefield L, Mooney C, et al. Accuracy of in-utero MRI to detect fetal brain abnormalities and prognosticate developmental outcome: postnatal follow-up of the MERIDIAN cohort. The Lancet Child & Adolescent Health. 2020;4(2):131-40. https://doi.org/10.1016/S2352-4642(19)30349-9 PMid:31786091 |
||||
| 24. Moradi B, Nezhad ZA, Saadat NS, Shirazi M, Borhani A, Kazemi MA. Apparent diffusion coefficient of different areas of brain in foetuses with intrauterine growth restriction. Polish Journal of Radiology. 2020;85:e301. https://doi.org/10.5114/pjr.2020.96950 PMid:32685065 PMCid:PMC7361370 |
||||
| 25. Levine D, McDonald RJ, Kressel HY. Gadolinium retention after contrast-enhanced MRI. Jama. 2018;320(18):1853-4. https://doi.org/10.1001/jama.2018.13362 PMid:30208489 |
||||
| 26. Sonigo PC, Rypens FF, Carteret M, Delezoide A-L, Brunelle FO. MR imaging of fetal cerebral anomalies. Pediatric radiology. 1998;28(4):212-22. https://doi.org/10.1007/s002470050335 PMid:9545473 |
||||
| 27. Van der Knoop B, Zonnenberg I, Verbeke J, De Vries L, Pistorius L, Van Weissenbruch M, et al. Additional value of advanced neurosonography and magnetic resonance imaging in fetuses at risk for brain damage. Ultrasound in Obstetrics & Gynecology. 2020;56(3):348-58. https://doi.org/10.1002/uog.21943 PMid:31828836 PMCid:PMC7496149 |
||||
| 28. Moradi B, Rahmani M, Kia K, Kazemi MA, Tahmasebpour A-R. Cavum velum interpositum cysts in normal and anomalous fetuses in second trimester of pregnancy: Comparison of its size and prevalence. Taiwanese Journal of Obstetrics and Gynecology. 2019;58(6):814-9. https://doi.org/10.1016/j.tjog.2019.09.016 PMid:31759534 |
||||
| Article View | 1,027 |
| PDF Download | 640 |