Document Type : Original Communication
Keywords
Introduction
In 2021, an estimated 6.2 million Americans aged 65 and older were affected by Alzheimer's disease (AD), contributing to $355 billion in total healthcare expenditures for individuals with dementia, as reported by the Alzheimer's Association. Projections suggest that by 2060, AD will impact 13.8 million Americans, underscoring its status as a significant public health challenge in the United States (1, 2). In June 2021, the U.S. Food and Drug Administration (FDA) approved aducanumab, a monoclonal antibody, marking it as the first disease-modifying treatment for AD (3). While aducanumab has demonstrated efficacy in reducing amyloid plaques (4), there remains considerable debate regarding whether amyloid clearance effectively mitigates cognitive and functional decline in patients (5). In light of these uncertainties, focusing on modifiable risk factors presents a promising approach to AD prevention. Increasing evidence suggests that neuroinflammation and blood clot formation are critical contributors to AD progression (6). Aspirin, or acetylsalicylic acid, is a widely utilized drug with anti-inflammatory and antiplatelet properties, making it a potential candidate for addressing these aspects of AD pathology (7).
The potential association between aspirin use and a reduced risk of AD may be attributed to its anti-inflammatory and cardioprotective effects (http://www.alzdiscovery.org). However, findings from observational studies and clinical trials have been inconsistent and, at times, contradictory. Etminan et al. (8), in a meta-analysis of three case-control and five cohort studies, found no significant association between aspirin use and the risk of developing AD. Conversely, Nilsson et al. (9), in a cross-sectional analysis, reported that high-dose aspirin significantly reduced the risk of AD in individuals aged 80 years and older. Similarly, Szekely et al. (10) combined data from six prospective studies and observed a reduced risk of AD among aspirin users. Subsequent large-scale prospective studies, however, have yielded mixed results, with reports indicating no effect (11, 12), an increased risk (13, 14), or a decreased risk (15, 16) of aspirin on AD development. The ASPREE (ASPirin in Reducing Events in the Elderly) clinical trial (17) found that low-dose aspirin was not associated with a reduced risk of developing AD in healthy elderly individuals. A recent observational study suggested that long-term low-dose aspirin use may slow the progression of AD in patients with coronary heart disease (CHD) but not in other populations. Additionally, a retrospective cohort study indicated that aspirin use may help prevent AD in patients with ischemic stroke (17). These divergent findings underscore the inherent limitations of observational studies, the heterogeneity of AD, and the possibility that aspirin may be associated with a decreased risk of AD in specific subpopulations that are not adequately represented in existing clinical trials.
|
Figure1. Box plot of FA values |
Diffusion tensor imaging (DTI) is a widely utilized in vivo neuroimaging technique for investigating white matter (WM) microstructure (18). By quantifying the diffusion of water molecules within tissues, DTI offers valuable insights into changes in WM integrity, such as axonal and myelin damage. In this study, we aimed to investigate the potential association between Aspirin use and WM microstructural changes quantified by DTI in a cohort of mild cognitive impairment (MCI) subjects.
Materials and Methods
Data Acquisition
Data were sourced from the Alzheimer's Disease Neuroimaging Initiative (ADNI) database (adni.loni.usc.edu). Established in 2003, the ADNI is a public–private partnership led by Principal Investigator Michael W. Weiner, MD. The primary objective of ADNI is to evaluate whether serial magnetic resonance imaging (MRI), positron emission tomography (PET), other biological markers, and clinical and neuropsychological assessments can effectively monitor the progression of MCI and early AD.
For this study, participants from the Alzheimer's Disease Neuroimaging Initiative phases ADNI2, ADNI3, and ADNIGO, who had baseline DTI measurements along with available demographic data, were initially selected. Due to the low number of cases, individuals with subjective memory concerns (SMC) were excluded. The final cohort included 148 MCI participants. All MCI participants were diagnosed with amnestic MCI based on the following criteria: a Mini-Mental State Examination (MMSE) score between 24 and 30, the presence of a memory complaint, objective memory impairment determined by education-adjusted scores on the Wechsler Memory Scale Logical Memory II, a Clinical Dementia Rating (CDR) of 0.5, no significant deficits in other cognitive domains, preservation of activities of daily living, and the absence of dementia.
Data regarding statin use were extracted from the ADNI concurrent medication file, which documents the longitudinal medication usage of participants. Individuals who had used Aspirin for a minimum of three years were aspirin users. The duration of statin use was calculated by determining the interval between the start date of aspirin therapy and the date of the baseline visit.
DTI Processing and Image Analysis
The analysis of DTI regions of interest (ROI) was conducted using data from the ADNI cohort. DTI scans were standardized using the Montreal Neurological Institute and Hospital (MNI) nu_correct tool (www.bic.mni.mcgill.ca/software/). Non-brain tissues were excluded using the Brain Extraction Tool (BET) from FSL. The T1-weighted images were aligned to a modified version of the Colin27 brain template using FSL’s FLIRT [18]. The Colin27 brain was zero-padded to create a cubic isotropic image size (220 x 220 x 220 mm³), which was then down-sampled to 110 x 110 x 110 mm³ to match the resolution of the diffusion-weighted imaging (DWI). A single diffusion tensor was modeled at each voxel within the brain, generating scalar anisotropy and diffusivity maps from the diffusion tensor eigenvalues (λ1, λ2, λ3). Fractional anisotropy (FA), representing the directional dependence of water diffusion, and mean diffusivity (MD), radial diffusivity (RD), and axial diffusivity (AxD), reflecting the extent of diffusion, were computed. Decreased FA and increased RD, AxD, and MD values suggest demyelination and white matter degeneration.
A shared information-based elastic registration algorithm, as previously described, was utilized to align the FA images from the Johns Hopkins University (JHU) DTI atlas to each participant's brain. Nearest-neighbor interpolation was employed to apply deformation to the stereotaxic JHU "Eve" white matter atlas labels (http://cmrm.med.jhmi.edu/cmrm/atlas/human_data/file/Atlas Explanation2.htm), thereby ensuring accurate placement of atlas ROIs within the same coordinate space as the DTI maps. Subsequently, average FA and MD values were computed within the boundaries of each ROI mask for each participant.
Statistical Analysis
Statistical analyses were performed using SPSS Statistics version 16 (IBM Corp., Armonk, NY). Comparisons of clinical and demographic variables between groups stratified by aspirin exposure were conducted using the t-test for continuous variables and the chi-square test for categorical variables. Neuroimaging variables were log-transformed to ensure they met the criteria for normal distribution prior to analysis. The relationship between aspirin exposure and neuroimaging parameters was assessed using an analysis of covariance (ANCOVA) model, adjusted for age, sex, APOE ε4 genotype, and Mini-Mental State Examination (MMSE) score. To control for type I errors resulting from multiple comparisons, the Benjamini-Hochberg correction was applied.
|
Figure3. Box plot of RD values |
|
Figure2. Box plot of FA values |
Results
Patient demographic
This study comprised 148 MCI participants with a mean age of 75.2 (±7.6) years, of whom 82 were identified as aspirin users. There were no significant differences in clinical or demographic characteristics between aspirin users and non-users.
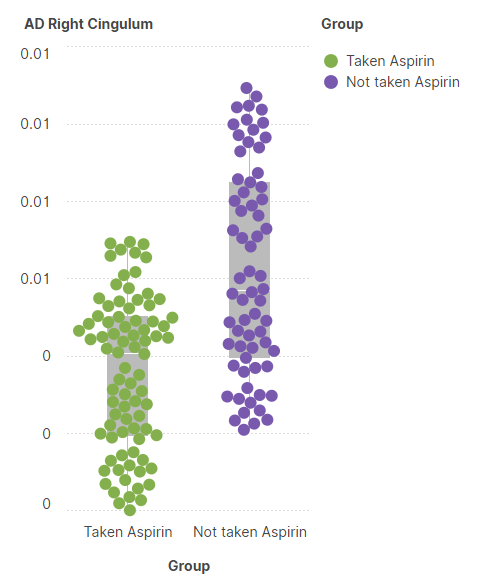
A univariate linear model was utilized to compare hippocampal and cortical volumes between aspirin users and non-users, adjusting for age, sex, and APOE ε4 genotype. The results from the univariate model revealed that aspirin users had significantly higher FA values in the anterior corona radiata (p < 0.001) (Figure 1) and the left external capsule (p = 0.003) (Figure 2). Moreover, the AD and RD values of the right cingulum were significantly lower in aspirin users compared to non-users (p < 0.001)(Figures 3 and 4).
Discussion
Although the precise etiology of AD remains largely undetermined, the "amyloid hypothesis" posits that impaired clearance of amyloid-beta protein plaques plays a key role in AD pathogenesis (19). Consequently, enhancing the brain's cellular pathways responsible for waste disposal may represent a promising approach to slowing or delaying the progression of AD. Transcription factor EB (TFEB) is known to regulate the expression of the brain's debris-clearing mechanisms. A previous study demonstrated that aspirin use upregulated TFEB, increased lysosome production, and reduced amyloid plaque pathology in AD model mice (20).
Epidemiological and clinical trial studies have produced inconsistent and often contradictory findings regarding the relationship between aspirin use and AD risk. These observational studies are vulnerable to residual confounding and bias. Moreover, the potential protective effects of aspirin on AD may be confined to specific subpopulations. For instance, previous observational studies have suggested that aspirin is associated with reduced cognitive decline in patients with stroke or coronary heart disease (CHD) in intensive care unit (ICU) (16, 21, 22). The ASPREE trial, which focused on healthy elderly participants (17), may have failed to detect the protective effects of aspirin on reducing AD risk in certain high-risk populations. Our study, utilizing summary genetic data from large-scale genome-wide association studies (GWAS), provides evidence that aspirin use may be causally linked to a decreased risk of AD, potentially mediated by factors such as CHD, blood pressure, and lipid levels. This suggests that aspirin could offer a more substantial protective effect in individuals at higher risk for CHD, depression, abnormal blood pressure, or lipid dysregulation (23).
|
Figure4. Box plot of AD values |
White matter, primarily composed of myelinated axons, plays a crucial role in maintaining cognitive function by facilitating communication between different regions of the brain (24). Inflammation, cancer and microvascular pathology are key contributors to white matter damage, leading to conditions such as white matter hyperintensities, which are associated with cognitive decline and neurodegenerative diseases, including AD (25, 26). White matter brain changes in Alzheimer's disease are pathologically associated with impairments in visual dual-task performance, reflecting the disruption of neural networks critical for multitasking and cognitive-motor integration (27). Emerging research suggests a potential association between tranexamic acid, Vitamin C, and Zinc and an increased risk of AD, although the underlying mechanisms and clinical significance of this relationship require further investigation (28, 29). Also, COVID-19 infection may be associated with white matter brain changes, including microstructural alterations and potential long-term impacts on cognitive function, though further research is needed to fully understand the extent and mechanisms of these changes (30-32). However, recent evidence suggests white matter damage due to the COVID-19 and other viral infections (33, 34). Pathological changes in white matter have been implicated in autism spectrum disorder, suggesting that disruptions in white matter integrity may underlie the atypical neural connectivity and cognitive impairments characteristic of the condition (35). Furthermore, other techniques such as quantitative ultrasound which has been explored as a non-invasive tool to detect pathological changes in brain white matter, with studies suggesting it may be sensitive to microstructural alterations linked to various neurodegenerative conditions (36, 37).
Aspirin, due to its anti-inflammatory and antithrombotic properties, has been investigated for its potential protective effects on white matter integrity. Some studies have suggested that aspirin may help preserve white matter health by reducing inflammation and preventing microvascular injury, which are critical factors in the development of white matter lesions. For instance, Bowman et al. found that aspirin use was associated with a reduction in the progression of white matter hyperintensities in elderly individuals (38). However, the results are not universally consistent, and further research is necessary to clarify aspirin's role in white matter health.
Conclusion
Aspirin is widely prescribed to millions of adults, yet its impact on WM regions in the brain remains largely unclear. In this study, we demonstrate that aspirin preserves WM microstructure in early AD. Although aspirin has been suggested as a potential therapeutic agent for neurodegenerative diseases, including AD, clinical trials have generally yielded negative results, likely due to the insufficient duration of therapy or the initiation of treatment after cognitive impairment has already developed. Further research is necessary to replicate these findings and to assess whether the effects of aspirin on WM structure could contribute to delaying or preventing cognitive decline.
Acknowledgments
Data collection and sharing for this project was funded by the Alzheimer's Disease Neuroimaging Initiative (ADNI) (National Institutes of Health Grant U01 AG024904) and DOD ADNI (Department of Defense award number W81XWH-12-2-0012). ADNI is funded by the National Institute on Aging, the National Institute of Biomedical Imaging and Bioengineering, and through generous contributions from the following: AbbVie, Alzheimer’s Association; Alzheimer’s Drug Discovery Foundation; Araclon Biotech; BioClinica, Inc.; Biogen; Bristol-Myers Squibb Company; CereSpir, Inc.; Cogstate; Eisai Inc.; Elan Pharmaceuticals, Inc.; Eli Lilly and Company; EuroImmun; F. Hoffmann-La Roche Ltd and its affiliated company Genentech, Inc.; Fujirebio; GE Healthcare; IXICO Ltd.; Janssen Alzheimer Immunotherapy Research & Development, LLC.; Johnson &
Johnson Pharmaceutical Research & Development LLC.; Lumosity; Lundbeck; Merck & Co., Inc.; Meso Scale Diagnostics, LLC.; NeuroRx Research; Neurotrack Technologies; Novartis Pharmaceuticals Corporation; Pfizer Inc.; Piramal Imaging; Servier; Takeda Pharmaceutical Company; and Transition Therapeutics. The Canadian Institutes of Health Research is providing funds to support ADNI clinical sites in Canada. Private sector contributions are facilitated by the Foundation for the National Institutes of Health (www.fnih.org). The grantee organization is the Northern California Institute for Research and Education, and the study is coordinated by the Alzheimer’s Therapeutic Research Institute at the University of Southern California. ADNI data are disseminated by the Laboratory for Neuro Imaging at the University of Southern California.
Declarations
Funding
We do not have any financial support for this study.
Conflict of interest
The authors have no conflicts of interest to disclose.
Availability of data
The datasets analyzed during the current study are available upon request with no restriction.
Code availability
Not applicable
Ethical approval
The data in this paper were obtained from the ADNI database (adni.loni.usc.edu). It does not include any examination of human or animal subjects.
Consent for publication
This manuscript has been approved for publication by all authors.
| 1. 2021 Alzheimer's disease facts and figures. Alzheimers Dement. 2021;17(3):327-406. https://doi.org/10.1002/alz.12328 PMid:33756057 |
||||
| 2. Entezami MaH, H. Green Drug Supply Chain Investigation by Time-Market Balance and Risk. World Journal of Engineering and Technology. 2023;11:611-31. https://doi.org/10.4236/wjet.2023.113042 |
||||
| 3. de la Torre JC, Gonzalez-Lima F. The FDA Approves Aducanumab for Alzheimer's Disease, Raising Important Scientific Questions1. J Alzheimers Dis. 2021;82(3):881-2. https://doi.org/10.3233/JAD-210736 PMid:34250943 |
||||
| 4. Sevigny J, Chiao P, Bussière T, Weinreb PH, Williams L, Maier M, et al. The antibody aducanumab reduces Aβ plaques in Alzheimer's disease. Nature. 2016;537(7618):50-6. https://doi.org/10.1038/nature19323 PMid:27582220 |
||||
| 5. Walsh S, Merrick R, Milne R, Brayne C. Aducanumab for Alzheimer's disease? Bmj. 2021;374:n1682. https://doi.org/10.1136/bmj.n1682 PMid:34226181 PMCid:PMC8258645 |
||||
| 6. Leng F, Edison P. Neuroinflammation and microglial activation in Alzheimer disease: where do we go from here? Nat Rev Neurol. 2021;17(3):157-72. https://doi.org/10.1038/s41582-020-00435-y PMid:33318676 |
||||
| 7. DiNicolantonio JJ, O'Keefe JH, Lavie CJ. Benefits and risks of aspirin use. Jama. 2012;308(11):1088-9; author reply 90. https://doi.org/10.1001/2012.jama.10717 PMid:22990257 |
||||
| 8. Etminan M, Gill S, Samii A. Effect of non-steroidal anti-inflammatory drugs on risk of Alzheimer's disease: systematic review and meta-analysis of observational studies. Bmj. 2003;327(7407):128. https://doi.org/10.1136/bmj.327.7407.128 PMid:12869452 PMCid:PMC165707 |
||||
| 9. Nilsson SE, Johansson B, Takkinen S, Berg S, Zarit S, McClearn G, et al. Does aspirin protect against Alzheimer's dementia? A study in a Swedish population-based sample aged > or =80 years. Eur J Clin Pharmacol. 2003;59(4):313-9. https://doi.org/10.1007/s00228-003-0618-y PMid:12827329 |
||||
| 10. Szekely CA, Green RC, Breitner JC, Østbye T, Beiser AS, Corrada MM, et al. No advantage of A beta 42-lowering NSAIDs for prevention of Alzheimer dementia in six pooled cohort studies. Neurology. 2008;70(24):2291-8. https://doi.org/10.1212/01.wnl.0000313933.17796.f6 PMid:18509093 PMCid:PMC2755238 |
||||
| 11. Kelley BJ, McClure LA, Unverzagt FW, Kissela B, Kleindorfer D, Howard G, et al. Regular aspirin use does not reduce risk of cognitive decline. J Am Geriatr Soc. 2015;63(2):390-2. https://doi.org/10.1111/jgs.13271 PMid:25688615 PMCid:PMC4339216 |
||||
| 12. Szekely CA, Breitner JC, Fitzpatrick AL, Rea TD, Psaty BM, Kuller LH, et al. NSAID use and dementia risk in the Cardiovascular Health Study: role of APOE and NSAID type. Neurology. 2008;70(1):17-24. https://doi.org/10.1212/01.wnl.0000284596.95156.48 PMid:18003940 PMCid:PMC2877629 |
||||
| 13. Waldstein SR, Wendell CR, Seliger SL, Ferrucci L, Metter EJ, Zonderman AB. Nonsteroidal anti-inflammatory drugs, aspirin, and cognitive function in the Baltimore longitudinal study of aging. J Am Geriatr Soc. 2010;58(1):38-43. https://doi.org/10.1111/j.1532-5415.2009.02618.x PMid:20122039 PMCid:PMC2832849 |
||||
| 14. Mandas A, Mereu RM, Catte O, Saba A, Serchisu L, Costaggiu D, et al. Cognitive Impairment and Age-Related Vision Disorders: Their Possible Relationship and the Evaluation of the Use of Aspirin and Statins in a 65 Years-and-Over Sardinian Population. Front Aging Neurosci. 2014;6:309. https://doi.org/10.3389/fnagi.2014.00309 PMid:25426067 PMCid:PMC4224124 |
||||
| 15. Côté S, Carmichael PH, Verreault R, Lindsay J, Lefebvre J, Laurin D. Nonsteroidal anti-inflammatory drug use and the risk of cognitive impairment and Alzheimer's disease. Alzheimers Dement. 2012;8(3):219-26. https://doi.org/10.1016/j.jalz.2011.03.012 PMid:22546354 |
||||
| 16. Nguyen TNM, Chen LJ, Trares K, Stocker H, Holleczek B, Beyreuther K, et al. Long-term low-dose acetylsalicylic use shows protective potential for the development of both vascular dementia and Alzheimer's disease in patients with coronary heart disease but not in other individuals from the general population: results from two large cohort studies. Alzheimers Res Ther. 2022;14(1):75. https://doi.org/10.1186/s13195-022-01017-4 PMid:35624487 PMCid:PMC9145441 |
||||
| 17. Ryan J, Storey E, Murray AM, Woods RL, Wolfe R, Reid CM, et al. Randomized placebo-controlled trial of the effects of aspirin on dementia and cognitive decline. Neurology. 2020;95(3):e320-e31. https://doi.org/10.1212/WNL.0000000000009277 |
||||
| 18. Alger JR. The diffusion tensor imaging toolbox. J Neurosci. 2012;32(22):7418-28. https://doi.org/10.1523/JNEUROSCI.4687-11.2012 PMid:22649222 PMCid:PMC3444512 |
||||
| 19. Hardy J, Selkoe DJ. The amyloid hypothesis of Alzheimer's disease: progress and problems on the road to therapeutics. Science. 2002;297(5580):353-6. https://doi.org/10.1126/science.1072994 PMid:12130773 |
||||
| 20. Chandra S, Jana M, Pahan K. Aspirin Induces Lysosomal Biogenesis and Attenuates Amyloid Plaque Pathology in a Mouse Model of Alzheimer's Disease via PPARα. J Neurosci. 2018;38(30):6682-99. https://doi.org/10.1523/JNEUROSCI.0054-18.2018 PMid:29967008 PMCid:PMC6067079 |
||||
| 21. Douiri A, McKevitt C, Emmett ES, Rudd AG, Wolfe CD. Long-term effects of secondary prevention on cognitive function in stroke patients. Circulation. 2013;128(12):1341-8. https://doi.org/10.1161/CIRCULATIONAHA.113.002236 PMid:23935013 |
||||
| 22. Fathi M, Moghaddam NM, Jahromi SN. A prognostic model for 1-month mortality in the postoperative intensive care unit. Surgery Today. 2022;52(5):795-803. https://doi.org/10.1007/s00595-021-02391-6 PMid:34698938 |
||||
| 23. Movahed F, Heidari E, Sadeghi D, Rezaei Nejad A, Abyaneh R, Zarei M, et al. Incident diabetes in adolescents using antidepressant: a systematic review and meta-analysis. European Child & Adolescent Psychiatry. 2024. https://doi.org/10.1007/s00787-024-02502-x PMid:38914830 |
||||
| 24. Ghayedi Z, Banihashemian K, Shirdel S, Adineh Salarvand R, Zare M, zeinali s, et al. A Review of the Comparison of Working Memory Performance, Cognitive Function, and Behavioral, and Psychological Symptoms across Normal Aging, Mild Cognitive Impairment, and Alzheimer's Disease. Neurology Letters. 2024;3(Special Issue (Diagnostic and Therapeutic advances in Neurodegenerative diseases)):26-38. | ||||
| 25. Prins ND, Scheltens P. White matter hyperintensities, cognitive impairment and dementia: an update. Nat Rev Neurol. 2015;11(3):157-65. https://doi.org/10.1038/nrneurol.2015.10 PMid:25686760 |
||||
| 26. Farrokhi M, Taheri F, Farrokhi M, Heydari Z, Darbani R, Salbi M, et al. Advancements and Innovations in Cancer Management: A Comprehensive Perspective. Kindle. 2024;4(1):1-161. | ||||
| 27. Ghamari N, Ghaderpanah R, Sadrian SH, Fallah N. Effect of a visual dual task on postural stability-A comparative study using linear and nonlinear methods. Health Science Reports. 2023;6(8):e1437. https://doi.org/10.1002/hsr2.1437 PMid:37520463 PMCid:PMC10375842 |
||||
| 28. Ghorbani M, Sadrian SH, Ghaderpanah R, Neitzke CC, Chalmers BP, Esmaeilian S, et al. Tranexamic acid in total hip arthroplasty: An umbrella review on efficacy and safety. Journal of Orthopaedics. 2024;54:90-102. https://doi.org/10.1016/j.jor.2024.03.010 PMid:38560591 |
||||
| 29. Yousefian M, Abedimanesh S, Yadegar A, Nakhjavani M, Bathaie SZ. Co-administration of "L-Lysine, Vitamin C, and Zinc" increased the antioxidant activity, decreased insulin resistance, and improved lipid profile in streptozotocin-induced diabetic rats. Biomedicine & Pharmacotherapy. 2024;174:116525. https://doi.org/10.1016/j.biopha.2024.116525 PMid:38599057 |
||||
| 30. M. Mahdavimanshadi MGA, M. Mowlai and Z. Ahmadirad. A Multistage Stochastic Optimization Model for Resilient Pharmaceutical Supply Chain in COVID-19 Pandemic Based on Patient Group Priority,. 2024 Systems and Information Engineering Design Symposium (SIEDS), Charlottesville, VA, USA2024. p. 382-7. https://doi.org/10.1109/SIEDS61124.2024.10534683 |
||||
| 31. Rahimian Z, Feili A, Ghaderpanah R, Sadrian S, Hosseini SA, Ranjbar M, et al. COVID-19-associated acute pancreatitis: a systematic review of case reports. Przegląd Epidemiologiczny - Epidemiological Review. 2023;77(1):66-73. https://doi.org/10.32394/pe.77.07 PMid:37283284 |
||||
| 32. Ebrahimi B, Nazarinia M, Molayem M, Javidialsaadi A, Nemati M. Assessment of COVID-19-Associated Stress and Knowledge Among Iranian Population: A Web-Based Cross-sectional Survey. Arch Clin Infect Dis. 2022;17(2):e105980. https://doi.org/10.5812/archcid-105980 |
||||
| 33. Rajabipoor Meybodi A, Mohammadi M, Arjmandi H. A qualitative approach to the ethical challenges of Iranian nurses during the COVID-19 pandemic. Journal of Preventive and Complementary Medicine. 2022;1(3):156-62. | ||||
| 34. Movahed F, Darzi S, Mahdavi P, Salih Mahdi M, Qutaiba BAO, Naji Sameer H, et al. The potential use of therapeutics and prophylactic mRNA vaccines in human papillomavirus (HPV). Virol J. 2024;21(1):124. https://doi.org/10.1186/s12985-024-02397-9 PMid:38822328 PMCid:PMC11143593 |
||||
| 35. Montazeri Ghahjavarestani A, Haghighat-Manesh E, Atashpanjeh H, Behfar A, Zeynali S, Ghahri Lalaklou Z. An investigation into the social and behavioral interactions of kids with autism and their perspectives on the topic of sensory training. Neurology Letters. 2024;3(2):5-12. | ||||
| 36. McFarlin BL, Villegas-Downs M, Mohammadi M, Han A, Simpson DG, O'Brien WD. Enhanced identification of women at risk for preterm birth via quantitative ultrasound: a prospective cohort study. American Journal of Obstetrics & Gynecology MFM. 2024;6(5, Supplement):101250. https://doi.org/10.1016/j.ajogmf.2023.101250 PMid:38070676 |
||||
| 37. Sharbaf FR, Movahed, F., Pirjani, R., Teimoory, N., Shariat, M., & Farahani, Z. Comparison of fetal middle cerebral artery versus umbilical artery color Doppler ultrasound for predicting neonatal outcome in complicated pregnancies with fetal growth restriction. Biomedical Research and Therapy. 2018;5(5):2296-304. https://doi.org/10.15419/bmrat.v5i5.443 |
||||
| 38. Bowman GL, Silbert LC, Howieson D, Dodge HH, Traber MG, Frei B, et al. Nutrient biomarker patterns, cognitive function, and MRI measures of brain aging. Neurology. 2012;78(4):241-9. https://doi.org/10.1212/WNL.0b013e3182436598 PMid:22205763 PMCid:PMC3280054 |
||||

| Article View | 1,312 |
| PDF Download | 748 |
.%5B2%5D.PNG)
.%5B2%5D.PNG)
.%5B2%5D.PNG)