Document Type : Review Article
Keywords
Subjects
Introduction
Multiple sclerosis (MS) is an autoimmune disease of many regions of the central nervous system characterized by inflammatory demyelination and axonal damage that causes many symptoms such as motor, sensory, visual, and autonomic disorders, impairs physical functions and balance (1). Tremor, coordination disorder, muscle weakness, sensory disorders, and spasticity seen in patients with MS have been found to decrease dual-task performance (1).
Physiotherapy is one of the most important rehabilitation options and frequently used for managing symptoms in patients with MS (2). It is critical that the neuro-rehabilitation interventions should comprehensively manage and control many symptoms of neurologic patients. New technological-based approach has provided new possibilities for neuro-rehabilitation (3,4). Along with technological developments, the various symptoms in MS could be managed. Here, the purpose is reaching to the important principle of neuro-rehabilitation and motor learning as the "concept of practice" that should contain 3 main characteristics modified for MS: optimal intensity, optimal repetition, and function, that induce neuroplastic changes and motor recovery in patients with MS (4). Technology-based rehabilitation allows therapists to control the beginning, continuation and end of training in a planned way, and adjust the therapeutic parameters such as duration, intensity, and frequency of the treatments. It allows to create motivating background to convert the patients from a passive individual to an active participant (5).
On the other hand, based on many research increased in the last 10 years which still persists, given the fact that this approach is not used across the board in clinical routine. Despite being challenging in terms of cost and accessibility, it is promising and has enormous potential for the future to engage patients and their families in the development of technology for rehabilitation. The optimal therapeutic paradigm regarding technology-based rehabilitation in patients with MS, amount of treatment dosage, and duration still has to be established in order to maximize clinical effectiveness of intensive rehabilitation. However, doubts emerged that the underlying rationale of the inter- and multi-disciplinary models in intensive hospitalized rehabilitation may be unnecessary and postulates that leads to the potential overwork damages and unhelpful. Whilst, perhaps going even beyond the application of new technological rehabilitation with intensive rehabilitation may be achieved by applying brain stimulation approach like transcranial electrical stimulation (tES), virtual reality training (VRT), applying aerobic exercises during mechanotherapy, combination of exercise and electrotherapy and electro-mechanical components or robotic devices for gait training. As a result, this purpose is to describe what new neuro-rehabilitation practices focus on the principle of motor learning with high-intensity, repetitive and functional exercise training.
Recommendations for Intensive Rehabilitation
Transcranial Electrical Stimulation (tES)
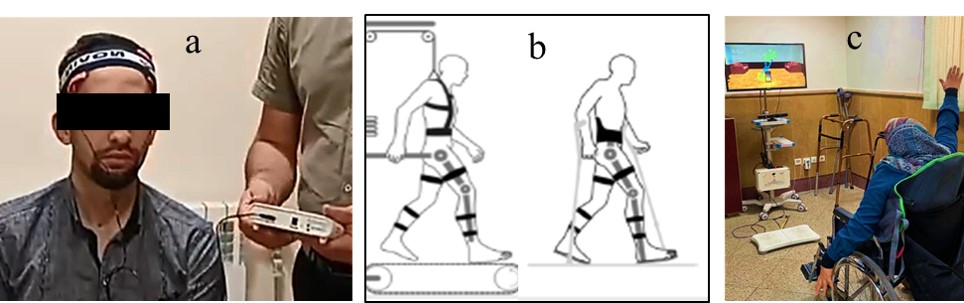
Transcranial Electrical Stimulation (tES), as a neuromodulation technique, consists of low intensity brain stimulation with applying a transcranial direct current stimulation (tDCS), or a transcranial alternating current stimulation (tACS) or a transcranial random noise stimulation (tRNS) using anode and cathode electrodes (Figure 1a). The tES could have short- and long-term effects due to underlying neuronal mechanisms including change in membrane polarization, prolonged opening of the voltage-gated sodium channels, neuro-transmitters releases, neurogenesis, more synaptic connectivity, cortical reorganization and eventually neuroplasticity (6,7). The tDCS application in symptoms of the patients with MS focused on fatigue reduction when targeting the prefrontal or sensorimotor cortex (8,9). tDCS also appear to be effective method for pain through stimulation of the left dorsolateral prefrontal, as a critical zone in pain processing, and primary motor cortex (M1) with an antidromic modulation of thalamocortical pathways (7,10). Finally, it seems coupling tES and other therapeutic interventions would help improve the symptoms in the patients with MS.
Robotic Devices for Gait Training
A commonly reported criteria of the disease progression in MS patients is the slower walking speed and worse gait quality with more energy consumption. For this reason, a potential benefit from exercise training in severe disability conditions of MS patients towards improving mobility is essential. Usually, the gait disability presents a sensory deficit, lack of muscle strength, impaired muscle control, and reduced aerobic capacity (Figure 1b).
However, few studies have shown that robotic rehabilitation was more effective than conventional methods in functional mobility, cognitive processing, and improvement of daily activities, gait parameters (11,12), but conceptually, robotic rehabilitation can help individuals with MS disability actively engage in exercise training by correcting impaired gait patterns (13,14). A key characteristic of robotic rehabilitation is that it promotes motor recovery within an enriched sensorimotor network for neuroplasticity as a primary mechanism (15). A beneficial changes in mobility, fatigue, and quality of life have been reported with treadmill training while body weight support (16,17). Also, an improvement of extensor muscle strength in the lower limbs, walking endurance, and fatigue were conducted with an robotic exoskeleton (18,19). However, the robotic devices used in spastic patients should have an active assisted movement when the patient cannot complete the active movement and have active resistance exercise mode.
Virtual Reality Training (VRT)
Virtual Reality (VR) as a simulation system, allows interaction between the patient and computer- constructed environment with the feeling of moving in the real world (Figure 1c). The main advantage of VRT is multi-sensory input and feedback including somatosensory, visual and auditory, that is suitable for motor learning with high-intensity, motivation of patient and enhancing active participation of the patient in the treatment regimen with a positive attitude, and simplifying complex movements. However, it is possible to create a headache, disorientation, lethargy, fatigue, ataxia and vertigo in the immersive type of VRT (4,20).
The role of VRT as a rehabilitation method in MS patients, has been discussed in the literature. Many studies have reported that VRT may significantly improve motor ability and cognitive functions, and can recover functional deficiencies in patients with MS (21–23). Furthermore, VRT can affect fatigue, fear of falling, balance disorders (24,25). Also, VRT interestingly has a sensory-integration optimization in the central nervous system (26).
Exercise Training with Electrical Stimulation
Many evidence state MS patients experience various symptoms such as fatigue, weakness and poor conditioning that likely limit the engagement of patients in physical activity, exacerbated by the association of physical inactivity with an
|
Figure 1. Examples of the new technological-based approaches for physical therapy in MS; a) Transcranial Electrical Stimulation (tES), b) Robotic Devices for Gait Training and c) Virtual Reality Training (VRT).
|
increased relative risk of cardiovascular and metabolic diseases (27). Therefore, exercise therapy and physical training will be important in these patients for designing effective intensive rehabilitation, either in the form of aerobic, endurance, or resistance exercise training. Additionally, the application of functional training programs has underlined the necessity of a multidimensional protocol regarding conventional protocols. Specially, the combination of task-oriented and functional training with aerobic exercise, has been shown to improve balance and walking indexes (28).
On the other hand, the application of electrically powered cycling with the assistance of functional electrical stimulation (FES) is a promising method for improving function without an increase in spasticity, fatigue and pain in people with MS who need a wheelchair for mobility (29,30). FES cycling is potentially helpful intervention for increasing physical activity level, as well as reducing fatigue and improving capacity of neuromuscular conditioning, based on clinical characteristics and progressive status of MS). FES cycle training improves symptoms of spasticity but approximately 48 hours after training (31,32). However, cycling is basically considered to be aerobic, stimulate modest increases in muscular strength (33). Actually, to strengthen skeletal muscle in healthy people with aerobic training, the efficient intensity should be as a minimum of 70% heart rate reserve, four-times a week for thirty minutes. Also, FES is applied peripherally to the nerve supply of weak foot extensors muscles to prevent foot drop and recover function and improvement in walking speed (30,34).
Bio-Feedback Training
In bio-feedback therapy, body signals are exposed to the patients in real-time, so that the person with perception of physical processes, can learn how to affect the output functions in order to improve the mental, psychosomatic and physical situations (35). Jensen et al. (36) showed a positive influence on the chronic pain in MS patients using EEG-based biofeedback therapy. Prosperini et al. (37) investigated the effects of visual-sensorimotor biofeedback training on risk of falling in patients with MS, while visual feedback of their postural control on a balance board was displayed. They reported a significant increase in postural stability and a significant reduction of falls after six weeks of training.
The biofeedback therapy would be effective with measuring the breathing rate and muscle tension, causing reductions in self-reported fatigue, especially when combined with training in mindful breathing awareness to increase regulation of emotion. Promisingly, for relapse-remit courses in MS patients the biofeedback therapy was shown to be effective in reducing anxiety, fatigue, and stress. There was also a trend toward significant reduction of breathing rate and muscle tension in favor of biofeedback (38).
Conclusion and Future Directions
Numerous studies have presented the standards of physiotherapeutic methods in MS. Intensive inpatient rehabilitation and usage of goal-oriented training seems to be more efficient and plays an important role in neuro-rehabilitation. The role of daily inpatient rehabilitation, which is related to the functional situation of the patient, has been concentrated on the cardiopulmonary, neuromuscular, musculoskeletal, and psychosocial status. Intensive rehabilitation provides many advantages for functional training, motor learning and implementation of practice concept. However, it is recommended that therapists with proper clinical experience apply these approaches and seek them for the patients.
Acknowledgments
I would like to thank the Clinical Research Development Center of Rofeideh Rehabilitation Hospital, Tehran, Iran for their support and assistance.
Deceleration
Funding
We do not have any financial support for this study.
Conflict of interest
The authors declare no conflict of interest regarding the publication of this paper.
Availability of data and material
The datasets analyzed during the current study are available upon request with no restriction.
Consent for publication
This manuscript has been approved for publication by all authors.
| 1. Vercellino M, Masera S, Lorenzatti M, Condello C, Merola A, Mattioda A, et al. Demyelination, inflammation, and neurodegeneration in multiple sclerosis deep gray matter. J Neuropathol Exp Neurol. 2009;68(5):489-502. https://doi.org/10.1097/NEN.0b013e3181a19a5a PMid:19525897 |
||||
| 2. Kubsik-Gidlewska AM, Klimkiewicz P, Klimkiewicz R, Janczewska K, Woldańska-Okońska MZ. Rehabilitation in multiple sclerosis. Adv Clin Exp Med. 2017;26(4). https://doi.org/10.17219/acem/62329 PMid:28691412 |
||||
| 3. Mikolajczyk T, Ciobanu I, Badea DI, Iliescu A, Pizzamiglio S, Schauer T, et al. Advanced technology for gait rehabilitation: An overview. Adv Mech Eng. 2018;10(7):1687814018783627. https://doi.org/10.1177/1687814018783627 |
||||
| 4. Karakas H, Seebacher B, Kahraman T. Technology-Based Rehabilitation in People with Multiple Sclerosis: A Narrative Review. J Mult Scler Res. 2021;1(3):54-68. https://doi.org/10.4274/jmsr.galenos.2021.2021-10-3 |
||||
| 5. Calabrò RS, Russo M, Naro A, De Luca R, Leo A, Tomasello P, et al. Robotic gait training in multiple sclerosis rehabilitation: Can virtual reality make the difference? Findings from a randomized controlled trial. J Neurol Sci. 2017;377:25-30. https://doi.org/10.1016/j.jns.2017.03.047 PMid:28477702 |
||||
| 6. Ayache SS, Chalah MA. Neuroimaging and neuromodulation of invisible symptoms in multiple sclerosis. Front Hum Neurosci. 2024;18:1376095. https://doi.org/10.3389/fnhum.2024.1376095 PMid:38454906 PMCid:PMC10917909 |
||||
| 7. Palm U, Chalah MA, Padberg F, Al-Ani T, Abdellaoui M, Sorel M, et al. Effects of transcranial random noise stimulation (tRNS) on affect, pain and attention in multiple sclerosis. Restor Neurol Neurosci. 2016;34(2):189-99. https://doi.org/10.3233/RNN-150557 PMid:26890095 |
||||
| 8. Ayache SS, Chalah MA. The place of transcranial direct current stimulation in the management of multiple sclerosis-related symptoms. Neurodegener Dis Manag. 2018;8(6):411-22. https://doi.org/10.2217/nmt-2018-0028 PMid:30451080 |
||||
| 9. Ferrucci R, Vergari M, Cogiamanian F, Bocci T, Ciocca M, Tomasini E, et al. Transcranial direct current stimulation (tDCS) for fatigue in multiple sclerosis. Neuro-rehabilitation. 2014;34(1):121-7. https://doi.org/10.3233/NRE-131019 PMid:24284464 |
||||
| 10. Zucchella C, Mantovani E, De Icco R, Tassorelli C, Sandrini G, Tamburin S. Non-invasive brain and spinal stimulation for pain and related symptoms in multiple sclerosis: a systematic review. Front Neurosci. 2020;14:547069. https://doi.org/10.3389/fnins.2020.547069 https://doi.org/10.3389/fnins.2020.00729 |
||||
| 11. Androwis GJ, Sandroff BM, Niewrzol P, Fakhoury F, Wylie GR, Yue G, et al. A pilot randomized controlled trial of robotic exoskeleton-assisted exercise rehabilitation in multiple sclerosis. Mult Scler Relat Disord. 2021;51:102936. https://doi.org/10.1016/j.msard.2021.102936 PMid:33878619 |
||||
| 12. Sconza C, Negrini F, Di Matteo B, Borboni A, Boccia G, Petrikonis I, et al. Robot-assisted gait training in patients with multiple sclerosis: a randomized controlled crossover trial. Medicina (B Aires). 2021;57(7):713. https://doi.org/10.3390/medicina57070713 PMid:34356994 PMCid:PMC8306232 |
||||
| 13. Androwis GJ, Pilkar R, Ramanujam A, Nolan KJ. Electromyography assessment during gait in a robotic exoskeleton for acute stroke. Front Neurol. 2018;9:262008. https://doi.org/10.3389/fneur.2018.00630 PMid:30131756 PMCid:PMC6090052 |
||||
| 14. Ramanujam A, Cirnigliaro CM, Garbarini E, Asselin P, Pilkar R, Forrest GF. Neuromechanical adaptations during a robotic powered exoskeleton assisted walking session. J Spinal Cord Med. 2018;41(5):518-28. https://doi.org/10.1080/10790268.2017.1314900 PMid:28427305 PMCid:PMC6117573 |
||||
| 15. Bonanno L, Russo M, Bramanti A, Calabrò RS, Marino S. Functional connectivity in multiple sclerosis after robotic rehabilitative treatment: A case report. Medicine (Baltimore). 2019;98(17):e15047. https://doi.org/10.1097/MD.0000000000015047 PMid:31027053 PMCid:PMC6831415 |
||||
| 16. Giesser B, Beres-Jones J, Budovitch A, Herlihy E, Harkema S. Locomotor training using body weight support on a treadmill improves mobility in persons with multiple sclerosis: a pilot study. Mult Scler J. 2007;13(2):224-31. https://doi.org/10.1177/1352458506070663 PMid:17450642 |
||||
| 17. Pilutti LA, Lelli DA, Paulseth JE, Crome M, Jiang S, Rathbone MP, et al. Effects of 12 weeks of supported treadmill training on functional ability and quality of life in progressive multiple sclerosis: a pilot study. Arch Phys Med Rehabil. 2011;92(1):31-6. https://doi.org/10.1016/j.apmr.2010.08.027 PMid:21187202 |
||||
| 18. Beer S, Aschbacher B, Manoglou D, Gamper E, Kool J, Kesselring J. Robot-assisted gait training in multiple sclerosis: a pilot randomized trial. Mult Scler J. 2008;14(2):231-6. https://doi.org/10.1177/1352458507082358 PMid:17942510 |
||||
| 19. Straudi S, Fanciullacci C, Martinuzzi C, Pavarelli C, Rossi B, Chisari C, et al. The effects of robot-assisted gait training in progressive multiple sclerosis: a randomized controlled trial. Mult Scler J. 2016;22(3):373-84. https://doi.org/10.1177/1352458515620933 PMid:26658817 |
||||
| 20. LaViola Jr JJ. A discussion of cybersickness in virtual environments. ACM Sigchi Bull. 2000;32(1):47-56. https://doi.org/10.1145/333329.333344 |
||||
| 21. Lozano-Quilis J-A, Gil-Gómez H, Gil-Gómez J-A, Albiol-Pérez S, Palacios-Navarro G, Fardoun HM, et al. Virtual rehabilitation for multiple sclerosis using a kinect-based system: randomized controlled trial. JMIR serious games. 2014;2(2):e2933. https://doi.org/10.2196/games.2933 PMid:25654242 PMCid:PMC4307818 |
||||
| 22. Lamargue-Hamel D, Deloire M, Saubusse A, Ruet A, Taillard J, Philip P, et al. Cognitive evaluation by tasks in a virtual reality environment in multiple sclerosis. J Neurol Sci. 2015;359(1-2):94-9. https://doi.org/10.1016/j.jns.2015.10.039 PMid:26671094 |
||||
| 23. Jonsdottir J, Bertoni R, Lawo M, Montesano A, Bowman T, Gabrielli S. Serious games for arm rehabilitation of persons with multiple sclerosis. A randomized controlled pilot study. Mult Scler Relat Disord. 2018;19:25-9. https://doi.org/10.1016/j.msard.2017.10.010 PMid:29112939 |
||||
| 24. Nascimento AS, Fagundes CV, dos Santos Mendes FA, Leal JC. Effectiveness of virtual reality rehabilitation in persons with multiple sclerosis: a systematic review and meta-analysis of randomized controlled trials. Mult Scler Relat Disord. 2021;54:103128. https://doi.org/10.1016/j.msard.2021.103128 PMid:34280679 |
||||
| 25. Casuso-Holgado MJ, Martín-Valero R, Carazo AF, Medrano-Sánchez EM, Cortés-Vega MD, Montero-Bancalero FJ. Effectiveness of virtual reality training for balance and gait rehabilitation in people with multiple sclerosis: a systematic review and meta-analysis. Clin Rehabil. 2018;32(9):1220-34. https://doi.org/10.1177/0269215518768084 PMid:29651873 |
||||
| 26. Massetti T, Trevizan IL, Arab C, Favero FM, Ribeiro-Papa DC, de Mello Monteiro CB. Virtual reality in multiple sclerosis-a systematic review. Mult Scler Relat Disord. 2016;8:107-12. https://doi.org/10.1016/j.msard.2016.05.014 PMid:27456884 |
||||
| 27. Motl RW, McAuley E, Snook EM. Physical activity and multiple sclerosis: a meta-analysis. Mult Scler J. 2005;11(4):459-63. https://doi.org/10.1191/1352458505ms1188oa PMid:16042230 |
||||
| 28. Chasiotis AK, Kitsos DK, Stavrogianni K, Giannopapas V, Papadopoulou M, Zompola C, et al. Rehabilitation on cerebellar ataxic patients with multiple sclerosis: A systematic review. J Neurosci Res. 2023;101(12):1773-80. https://doi.org/10.1002/jnr.25235 PMid:37621200 |
||||
| 29. Backus D, Moldavskiy M, Sweatman WM. Effects of functional electrical stimulation cycling on fatigue and quality of life in people with multiple sclerosis who are nonambulatory. Int J MS Care. 2020;22(4):193-200. https://doi.org/10.7224/1537-2073.2019-101 PMid:32863788 PMCid:PMC7446631 |
||||
| 30. Pilutti LA, Motl RW. Functional electrical stimulation cycling exercise for people with multiple sclerosis. Curr Treat Options Neurol. 2019;21:1-13. https://doi.org/10.1007/s11940-019-0597-7 PMid:31705304 |
||||
| 31. Szecsi J, Schlick C, Schiller M, Pöllmann W, Koenig N, Straube A. Functional electrical stimulation-assisted cycling of patients with multiple sclerosis: biomechanical and functional outcome--a pilot study. J Rehabil Med. 2009;41(8):674-80. https://doi.org/10.2340/16501977-0397 PMid:19565162 |
||||
| 32. Krause P, Szecsi J, Straube A. FES cycling reduces spastic muscle tone in a patient with multiple sclerosis. Neuro-rehabilitation. 2007;22(4):335-7. https://doi.org/10.3233/NRE-2007-22412 PMid:17971625 |
||||
| 33. Konopka AR, Harber MP. Skeletal muscle hypertrophy after aerobic exercise training. Exerc Sport Sci Rev. 2014;42(2):53-61. https://doi.org/10.1249/JES.0000000000000007 PMid:24508740 PMCid:PMC4523889 |
||||
| 34. Learmonth YC, Rice IM, Ostler T, Rice LA, Motl RW. Perspectives on physical activity among people with multiple sclerosis who are wheelchair users: informing the design of future interventions. Int J MS Care. 2015;17(3):109-19. https://doi.org/10.7224/1537-2073.2014-018 PMid:26052256 PMCid:PMC4455863 |
||||
| 35. Giggins OM, Persson UM, Caulfield B. Biofeedback in rehabilitation. J Neuroeng Rehabil. 2013;10:1-11. https://doi.org/10.1186/1743-0003-10-60 PMid:23777436 PMCid:PMC3687555 |
||||
| 36. Jensen MP, Gianas A, George HR, Sherlin LH, Kraft GH, Ehde DM. Use of neurofeedback to enhance response to hypnotic analgesia in individuals with multiple sclerosis. Int J Clin Exp Hypn. 2016;64(1):1-23. https://doi.org/10.1080/00207144.2015.1099400 PMid:26599991 |
||||
| 37. Prosperini L, Leonardi L, De Carli P, Mannocchi ML, Pozzilli C. Visuo-proprioceptive training reduces risk of falls in patients with multiple sclerosis. Mult Scler J. 2010;16(4):491-9. https://doi.org/10.1177/1352458509359923 PMid:20150396 |
||||
| 38. Mackay AM, Buckingham R, Schwartz RS, Hodgkinson S, Beran RG, Cordato DJ. The effect of biofeedback as a psychological intervention in multiple sclerosis: a randomized controlled study. Int J MS Care. 2015;17(3):101-8. https://doi.org/10.7224/1537-2073.2014-006 PMid:26052255 PMCid:PMC4455862 |
||||

| Article View | 1,069 |
| PDF Download | 366 |