Document Type : Original Communication
Keywords
Subjects
Introduction
Stroke is a rapidly progressing local or widespread neurological disorder of cerebrovascular origin that lasts more than 24 hours or leads to death (1). A stroke can occur in the form of lack of blood supply to brain (ischemic) or intracerebral bleeding (hemorrhagic), which includes about 85% of ischemic and 15% of hemorrhagic cases (2). Stroke is one of the leading causes of long-term disability and the second leading cause of death worldwide (3, 4). This disease is the main cause of death in middle- and high-income countries, where about 6.7 million people died of stroke in United States in 2013 (5). Geographically, there is a great difference between the incidences of stroke deaths in the world. In Iran, the rate of stroke is higher than in western countries, which also occurs at a younger age. Ischemic stroke is more common than hemorrhagic stroke in Iran and its range is between 57.9% and 87% (6, 7). In addition, the index Disability-Adjusted Life Years (DALY) in these patients is generally about 51 million years (8, 9).
Most patients suffer from motor impairment after stroke, which affects their quality of life (10, 11). Thrombolytic therapy (as the only treatment proven to improve the outcome of such patients) is feasible only in a minority of clinical cases (12-14). Even with the use of this drug, more than half of IS patients are still disabled (15, 16). Despite the limited effectiveness of physical rehabilitation treatment methods, the possibility of recovery after stroke using pharmacological agents has always been attractive. These drugs act through different mechanisms and have the ability to improve function in many acute stroke survivors (17, 18). After a stroke, there are a variety of specific mechanisms that improve a person's motor status (19, 20). Based on animal and human studies, it has been hypothesized that the initial period after a stroke is the interval in which neural organization occurs, which indicates the existence of a sensitive period for the recovery of the patient's motor status (21). Pharmacological strategies in neurorehabilitation are mainly based on neuroplasticity, which is an inherent capacity of the brain's nervous system and allows continuous reorganization of the damaged neural network and restoration of its function in conditions such as stroke (22).
In the field of drug treatments, there are reports about the positive effects of selective serotonin reuptake inhibitors in the recovery of motor status after stroke (23-27). Although, there is logically convincing evidence for selective serotonin reuptake inhibitors, the case remains inconclusive. Some reports suggest that selective serotonin reuptake inhibitors may cause cerebral vasoconstriction and ischemic strokes (24). Furthermore, the risks or benefits of using selective serotonin reuptake inhibitors in the treatment of stroke patients are not fully understood (27). Although, fluoxetine has been extensively studied, there are promising positive data of citalopram in improving motor function in patients with acute stroke (12, 28). In Iranian society, studies show that citalopram is a safe and tolerable drug in patients with acute stroke, which can improve the final outcome in these patients (29). A study found that there was no significant difference between citalopram and fluoxetine in facilitating motor recovery after stroke in ischemic stroke patients. However, compared with placebo, both drugs improved motor function after stroke (30).
However, there are no sufficient findings for this case in clinical studies, especially in Iran (31-33). Since stroke is a disease that affects people's lives and causes a high economic and psychological burden for the patient and the treatment system, clinical studies have not fully confirmed or rejected the use or non-use of selective serotonin reuptake inhibitor drugs. Therefore, the aim was to investigate the effect of citalopram and fluoxetine on motor function after stroke in acute cerebral stroke patients referred to Shahid Beheshti Hospital in Kashan in 2021-2022.
Materials and Methods
Study Population
In this double-blind interventional study with placebo, 90 people diagnosed with acute cerebral stroke referred to the neurology department of Shahid Beheshti Hospital in Kashan in 2021-2022. After approved thesis and ethics code, informed consent was obtained from all patients before the intervention. Finally, those who were examined according to inclusion and exclusion criteria were included in the study. For these people, a basic Fugel-Meier movement scale score was assigned in order to compare with its final number. Considering the effect of depression in patients, two steps were taken to complete the demographic information and depression questionnaire (34).
Inclusion and Exclusion Criteria
The inclusion criteria included: age over 18 years, motor or sensory paralysis of half of the body following the first episode of acute stroke (within the last 24 hours), cerebral ischemia, and initial Vogel-Meier motor score below 55. Exclusion criteria also include: age over 70 years, National Institute of Health stroke score above 15 and previous disabilities such as: lack of speech, cognitive and movement disorders caused by stroke or any disease of the cerebral cortex, pregnancy or breastfeeding, current consumption of anti-depressant drugs.
Method
In the present study, the Beck II depression questionnaire was used to determine the severity of depression. This questionnaire is a 21-item self-assessment questionnaire that measures the severity of depression symptoms. Each substance (symptom of the disease) is divided into four degrees based on its severity and is scored from 0 to 3. A score of zero indicates the lowest level and a score of 3 indicates the highest level of intensity of experience, a sign of depression. The sum of the scores of each questionnaire can be between 0 and 63, which is used in people over 13 years old (34).
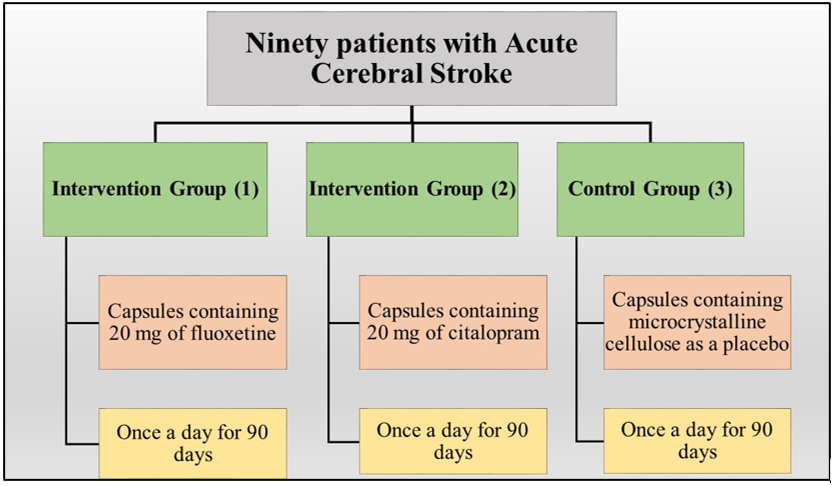
Ninety patients were randomly divided into 3 groups (30 people in each group) including A) fluoxetine, B) citalopram and C) placebo. All the drugs were produced by Dr. Abidi Company and were placed in a similar capsule by a pharmacist who was not aware of the randomization of the patients. Randomization was done into block randomization.
Intervention group 1: Participants received capsules containing 20 mg of fluoxetine orally once a day for 90 days and physiotherapy sessions based on stroke severity.
Intervention group 2: The participants received a capsule containing 20 mg of citalopram orally once a day for 90 days and physiotherapy sessions based on the severity of the stroke.
Control group 3: The participants received a capsule containing microcrystalline cellulose as a placebo in the form of food once a day for 90 days and received physiotherapy sessions based on the severity of the stroke (Figure 1).
|
Table 1. Distribution of demographic and clinical characteristics of patients in three groups in baseline. |
|||||
|
Variables |
Intervention Groups |
P-value |
|||
|
Fluoxetine |
Citalopram |
Placebo |
|||
|
Sex(M/F) |
19/11 |
20/10 |
19/11 |
0.95 |
|
|
Age (Years) |
62.13±8.99 |
62.77±7.4 |
61.07±7.75 |
0.71 |
|
|
Severity of Disability |
7.03±1.91 |
7.17±2.13 |
6.40±1.69 |
0.72 |
|
|
Beck's Depression Score |
9.50±4.85 |
9.13±4.87 |
8.73±5.51 |
0.84 |
|
|
Motor function score |
10.70±5.82 |
12.37±6.15 |
13.37±5.48 |
0.21 |
|
|
Motor performance score based on Meyer Fugl score |
1 month after intervention |
18.83±7.71 |
16.13±7.47 |
14.17±5.58 |
0.039 |
|
2 months after intervention |
32.13±8.29 |
27.43±6.97 |
18.63±5.84 |
<0.001 |
|
|
3 months after intervention |
52.80±13.33 |
50.00±13.76 |
27.63±3.76 |
<0.001 |
|
|
All the data in the table are shown as Mean±Standard Deviation (SD). |
|||||
The motor performance at the end of 90 days was measured by the researcher with the Vogel-Meyer motor scale. This test is designed based on Branstrom's concepts and stages of movement improvement. The test items include 50 movements in 6 recovery levels, of which 33 items are related to the upper limbs in the shoulder, elbow, forearm, wrist and hand (35).
Statistical Analysis
Data were analyzed after entering SPSS version 22 software. Quantitative variables were reported as mean and standard deviation (SD). To compare quantitative variables, t-test or Mann-Whitney test was used. Qualitative variables were compared using chi square test. Multiple logistic regression model was performed for the variables that were significantly different between groups according to univariate analysis.
Results
As seen in the table, there was no statistically significant difference in the frequency of gender in the patients of the three studied groups (P>0.05) (Table 1). The average age of the studied subjects was 61.99±8.02 years (34 to 70 years), of which 58 (64.4%) were men and 32 (35.6%) were women (Table 1). As seen in the table 1, the average age, severity of disability, Beck depression score, motor performance score based on Meyer Fugl score before the intervention in the patients of the three studied groups had no statistically significant difference (P>0.05).
The average motor function score based on Meyer Fugl score one month after the intervention was the highest value (18.83) in the fluoxetine group and the lowest value (14.17) in the placebo group. This difference was statistically significant (P=0.039). In a two-by-two comparison, it was found that there was a significant difference between fluoxetine and placebo, but no significant difference was seen between fluoxetine and citalopram and between citalopram and placebo.
The average motor function score based on Meyer Fugl score two months after the intervention was the highest value (32.13) in the fluoxetine group and the lowest value (18.63) in the placebo group, and this difference was statistically significant (P<0.001). In a two-by-two comparison, it was found that there was a significant difference between fluoxetine and placebo and citalopram and placebo (P<0.001). Also, a statistically significant difference was observed between fluoxetine and citalopram (P<0.05).
The average motor function score based on Meyer Fugl score three months after the intervention was the highest value (52.8) in the fluoxetine group and the lowest value (27.63) in the placebo group, and this difference was statistically significant (P<0.001). In a two-by-two comparison, it was found that there was a significant difference between fluoxetine and placebo and citalopram and placebo (P<0.001). However, there was no significant difference between fluoxetine and citalopram (P>0.05).
The results of Table 2 determined that the effect of time on the changes in motor function score was significant (P<0.05). This finding demonstrated that the performance score changes over time were the same in the three studied groups. In other words, the trend of score increase was seen in all three groups. Also, the effect of the three factors of the group time factor was seen in the significant performance score changes (P<0.05), which showed that the movement score changes over time are not the same and
|
Table 2. Results of ANOVA with repeated measures for the effects of time and treatment groups on motor performance score. |
|||||
|
Sig. |
F |
Mean Square |
df |
Type III |
Source |
|
Sum of Squares |
|||||
|
<0.001 |
510.23 |
32252.8 |
1.62 |
52311.5 |
Time |
|
<0.001 |
37.9 |
2396.1 |
3.24 |
7772.8 |
Time* group |
|
|
|
63.21 |
141.1 |
8919.5 |
Error |
are not equal to each other; In such a way that the trend of increase in fluoxetine and citalopram group was similar and higher than placebo group (P<0.05) (Table 2).
Discussion
Regarding to pharmacodynamics changes and the lack of evidence about the effects of different types of selective serotonin reuptake inhibitors on neurological recovery after stroke, the present study aimed to evaluate the effectiveness of oral citalopram, compared to fluoxetine and placebo in patients with motor disability after stroke. In this study, 90 patients were evaluated in three different groups.
The average motor function score based on Meyer Fugl score one, two and three months after the intervention was the highest in the fluoxetine group and the lowest in the placebo group. The motor function score based on this score during the follow-up and over time had a significant difference between the three groups.
While all previous studies have shown positive effects of selective serotonin reuptake inhibitors on motor recovery after stroke, (36-39) they have not compared these inhibitors with different pharmacodynamics. A recent systematic review failed to identify any selective serotonin inhibitor as superior to the others (40). All current studies have compared one type of selective serotonin reuptake inhibitor with placebo, with most of the data on fluoxetine. A well-designed study (the FLAME trial) showed that fluoxetine reduced motor impairment in patients with ischemic stroke and hemiplegia. Zittel et al in 2008 investigated the effects of a single dose of citalopram (40 mg) in 8 patients, six months after stroke, and found that the performance of the Nine-hole Peg hand test improved significantly (28). Acler et al (2009) investigated the effects of citalopram (10 mg p.o. daily for four months) in 20 patients with unilateral stroke in a randomized placebo-controlled study. They reported that patients treated with citalopram showed significant improvement in the National Institutes of Health Stroke Scale (41).
The innovation of our study is that it compares the effect of two selective serotonin reuptake inhibitors with different pharmacodynamics. Our findings indicated that citalopram, as a selective short-acting serotonin reuptake inhibitor, has similar effects to fluoxetine in facilitating post-stroke recovery and reducing stroke-related motor disability. During this period, no significant side effects were observed in the study subjects. A concern with selective serotonin reuptake inhibitor therapy is its potential to increase spasticity. However, after daily administration of fluoxetine or citalopram, our subjects did not experience spasticity.
Previously, fluoxetine was mainly used to treat depression, obsessive-compulsive disorder, and other mental disorders. Several animal studies have found mechanisms by which fluoxetine has the potential to improve motor performance (42-44). First, SSRIs can increase neurogenesis and neurotrophin expression in the hippocampus to have beneficial effects on the behavior of rats (25, 45). According to an animal study, SSRIs promote neurogenesis in the hippocampus and subventricular zone in the ventricular canal in rats where neurogenesis normally occurs (46). In addition, SSRI-mediated neurogenesis may contribute to structural and functional recovery after cerebral ischemia and the migration of new neurons from the neurogenic region to the damaged region (47, 48). Neurotrophins are proteins that cause organogenesis and embryogenesis and neural plasticity (49). Also, SSRIs may have the ability to protect neurons by inhibiting inflammatory responses through inhibition of microglia and neutrophils (50, 51). Inflammation is the main cause of brain cell damage in the later stages of stroke (51, 52). When inflammation damages brain cells, SSRIs reduce the number of cytotoxic inflammatory molecules by reducing the expression of microglia and neutrophils to protect brain cells from inflammatory damage. Animal experiments have shown that 9 hours after stroke in rats using an SSRI, there is still a significant improvement in the volume of the brain damaged area and in the neurological function compared to the control group (53). This finding supports the idea that SSRIs improve neuronal function in mice. Additionally, SSRIs may improve cerebral blood flow regulation by increasing the expression of Heme Oxygenase-1 (HO-1) and Hypoxia-Inducible Factor-1 alpha (HIF-1alpha) (54). An animal study showed that SSRIs increase the expression of HO-1, which in turn leads to the production of carbon monoxide to regulate vascular tone independently of pathways related to nitric oxide synthase (55). Finally, animal studies have shown increased β-1 adrenergic receptor expression in damaged rat brain regions after administration of SSRIs (50), which may improve performance. On the other hand, recent clinical trials have shown that citalopram treatment increases motor recovery after stroke (12, 31, 41). However, the mechanisms behind this improvement in clinical performance have not been elucidated.
SSRIs, such as citalopram, are permeable to the blood-brain barrier and are designed to enhance monoaminergic neurotransmitters in synaptic clefts (56). Increased serotonin leads to time-dependent changes in neurotrophic factors, i.e. BDNF becomes (57). According to the neurotrophin theory of depression, downstream activation of BDNF-regulated signaling pathways is a major mediator of the antidepressant effect of SSRIs (56). BDNF may play a positive role in the
|
Figure 1. Flow diagram: randomization and patient flowchart.
|
survival and migration of SVZ-derived neural progenitors. The observed migration to the peri-infarct area is a normal response to focal ischemia. This endogenous response was enhanced at 7 days with citalopram treatment (58, 59). The increase of neural progenitor cells in the migratory pathway in citalopram-treated animals along with the motor recovery seen at 14 days after stroke suggests that neurogenesis may play an important role in motor recovery. Increased endogenous migration in citalopram-treated rats may explain why functional improvement is observed 14 days after stroke. Furthermore, post-ischemic administration of citalopram increases BDNF protein expression in the peri-infarct cortex after 7 days and increases the number of new neurons in the peri-infarct region after 21 and 28 days of treatment (60).
SSRIs are FDA-approved, inexpensive, clinically available, and safe medications used in both depressed and nondepressed stroke patients (61, 62). This study showed that post-stroke treatment significantly increased the motor performance of non-depressed patients. This study shows that antidepressant treatment can modify the risk of post-stroke disability due to cardiovascular diseases and recurrent strokes (63). Potential side effects of Celexa (citalopram hydrobromide) as reported by the FDA include serotonin syndrome, which can cause rapid heart rate and high or low blood pressure, among several other symptoms. However, as measured by several clinical trials for stroke and depression, citalopram does not significantly increase blood pressure or pulse rate (64).
Conclusion
The findings of the present study showed that the average motor function score based on Meyer Fugl score one, two and three months after the intervention was the highest in the fluoxetine group and the lowest in the placebo group, and this difference was statistically significant. In total, the three studied groups had a significant difference between the three groups in repeated measurements of the motor performance score based on the Meyer Fugl score during the follow-up and over time. Therefore, it was found that fluoxetine and citalopram treatment restores motor function and may provide sustained recovery after stroke.
Recommendation:
It is suggested to conduct similar studies with a larger sample size and in different places of the country on different people hospitalized with stroke. Also, socio-economic characteristics as well as other demographic characteristics on the effect of these two drugs in restoring motor function after stroke should be investigated.
Declarations
Funding
We do not have any financial support for this study.
Conflict of interest
The authors have no conflicts of interest to disclose.
Availability of data
The datasets analyzed during the current study are available upon request with no restriction.
Code availability
Not applicable
Consent for publication
This manuscript has been approved for publication by all authors.
| 1. Sacco RL, Kasner SE, Broderick JP, Caplan LR, Connors J, Culebras A, et al. An updated definition of stroke for the 21st century: a statement for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. 2013;44(7):2064-89. https://doi.org/10.1161/STR.0b013e318296aeca PMid:23652265 PMCid:PMC11078537 |
||||
| 2. Wiener C, Fauci A, Braunwald E, Kasper D, Hauser S, Longo D, et al. Harrisons Principles of Internal Medicine Self-Assessment and Board Review 18th Edition. 2012. | ||||
| 3. Go AS, Mozaffarian D, Roger VL, Benjamin EJ, Berry JD, Borden WB, et al. Heart disease and stroke statistics-2013 update: a report from the American Heart Association. Circulation. 2013;127(1):e6-e245. | ||||
| 4. Benjamin EJ, Muntner P, Alonso A, Bittencourt MS, Callaway CW, Carson AP, et al. Heart disease and stroke statistics-2019 update: a report from the American Heart Association. Circulation. 2019;139(10):e56-e528. | ||||
| 5. Mozaffarian D, Benjamin EJ, Go AS, Arnett DK, Blaha MJ, Cushman M, et al. Heart disease and stroke statistics-2016 update: a report from the American Heart Association. circulation. 2016;133(4):e38-e360. | ||||
| 6. Delbari A, Salman Roghani R, Tabatabaei SS, Rahgozar M, Lokk J. Stroke epidemiology and one-month fatality among an urban population in Iran. International Journal of Stroke. 2011;6(3):195-200. https://doi.org/10.1111/j.1747-4949.2010.00562.x PMid:21557803 |
||||
| 7. Ghandehari K. Epidemiology of stroke in Iran. Galen Medical Journal. 2016;5:3-9. https://doi.org/10.31661/gmj.v5iS1.588 https://doi.org/10.31661/gmj.v5i.588 |
||||
| 8. Fisher M, Norrving B. 1st Global Conference on Healthy Lifestyles and Non communicable diseases Control. Moscow April. 2011:28-9. | ||||
| 9. Steinwachs DM, Collins-Nakai RL, Cohn LH, Garson A, Wolk MJ. The future of cardiology: utilization and costs of care. Journal of the American College of Cardiology. 2000;35(4):1092-9. https://doi.org/10.1016/S0735-1097(00)00559-3 PMid:10732913 |
||||
| 10. Hendricks HT, Van Limbeek J, Geurts AC, Zwarts MJ. Motor recovery after stroke: a systematic review of the literature. Archives of physical medicine and rehabilitation. 2002;83(11):1629-37. https://doi.org/10.1053/apmr.2002.35473 PMid:12422337 |
||||
| 11. Siepmann T, Penzlin AI, Kepplinger J, Illigens BMW, Weidner K, Reichmann H, et al. Selective serotonin reuptake inhibitors to improve outcome in acute ischemic stroke: possible mechanisms and clinical evidence. Brain and behavior. 2015;5(10):e00373. https://doi.org/10.1002/brb3.373 PMid:26516608 PMCid:PMC4614057 |
||||
| 12. Chollet F, Tardy J, Albucher J-F, Thalamas C, Berard E, Lamy C, et al. Fluoxetine for motor recovery after acute ischaemic stroke (FLAME): a randomised placebo-controlled trial. The Lancet Neurology. 2011;10(2):123-30. https://doi.org/10.1016/S1474-4422(10)70314-8 PMid:21216670 |
||||
| 13. Burns JD, Green DM, Metivier K, DeFusco C. Intensive care management of acute ischemic stroke. Emergency medicine clinics of North America. 2012;30(3):713-44. https://doi.org/10.1016/j.emc.2012.05.002 PMid:22974646 |
||||
| 14. Blinzler C, Breuer L, Huttner HB, Schellinger PD, Schwab S, Köhrmann M. Characteristics and outcome of patients with early complete neurological recovery after thrombolysis for acute ischemic stroke. Cerebrovascular Diseases. 2011;31(2):185-90. https://doi.org/10.1159/000321869 PMid:21160181 |
||||
| 15. Pantoni L, Fierini F, Poggesi A. Thrombolysis in acute stroke patients with cerebral small vessel disease. Cerebrovascular Diseases. 2014;37(1):5-13. https://doi.org/10.1159/000356796 PMid:24355873 |
||||
| 16. Paul CL, Ryan A, Rose S, Attia JR, Kerr E, Koller C, et al. How can we improve stroke thrombolysis rates? A review of health system factors and approaches associated with thrombolysis administration rates in acute stroke care. Implementation Science. 2015;11(1):1-12. https://doi.org/10.1186/s13012-016-0414-6 PMid:27059183 PMCid:PMC4825073 |
||||
| 17. Chollet F, Cramer S, Stinear C, Kappelle L, Baron J, Weiller C, et al. Pharmacological therapies in post stroke recovery: recommendations for future clinical trials. Journal of neurology. 2014;261(8):1461-8. https://doi.org/10.1007/s00415-013-7172-z PMid:24221642 |
||||
| 18. Budhdeo S, Rajapaksa S. Functional recovery in cerebral palsy may be potentiated by administration of selective serotonin reuptake inhibitors. Medical Hypotheses. 2011;77(3):386-8. https://doi.org/10.1016/j.mehy.2011.05.026 PMid:21683532 |
||||
| 19. Chen R. Cohen LG Hallet M. Nervous system reorganization following injury//Neuroscience. 2002;111:761-73. https://doi.org/10.1016/S0306-4522(02)00025-8 PMid:12031403 |
||||
| 20. Di Filippo M, Tozzi A, Costa C, Belcastro V, Tantucci M, Picconi B, et al. Plasticity and repair in the post-ischemic brain. Neuropharmacology. 2008;55(3):353-62. https://doi.org/10.1016/j.neuropharm.2008.01.012 PMid:18359495 |
||||
| 21. Stroemer RP, Kent TA, Hulsebosch CE. Neocortical neural sprouting, synaptogenesis, and behavioral recovery after neocortical infarction in rats. Stroke. 1995;26(11):2135-44. https://doi.org/10.1161/01.STR.26.11.2135 PMid:7482662 |
||||
| 22. Engelter S. Safety in pharmacological enhancement of stroke rehabilitation. Eur J Phys Rehabil Med. 2013;49(2):261-7. | ||||
| 23. Chollet F. Pharmacologic approaches to cerebral aging and neuroplasticity: insights from the stroke model. Dialogues in clinical neuroscience. 2022. | ||||
| 24. Pariente J, Loubinoux I, Carel C, Albucher JF, Leger A, Manelfe C, et al. Fluoxetine modulates motor performance and cerebral activation of patients recovering from stroke. Annals of neurology. 2001;50(6):718-29. https://doi.org/10.1002/ana.1257 PMid:11761469 |
||||
| 25. Schmidt HD, Duman RS. The role of neurotrophic factors in adult hippocampal neurogenesis, antidepressant treatments and animal models of depressive-like behavior. Behavioural pharmacology. 2007;18(5-6):391-418. https://doi.org/10.1097/FBP.0b013e3282ee2aa8 PMid:17762509 |
||||
| 26. Gu S-C, Wang C-D. Early selective serotonin reuptake inhibitors for recovery after stroke: a meta-analysis and trial sequential analysis. Journal of Stroke and Cerebrovascular Diseases. 2018;27(5):1178-89. https://doi.org/10.1016/j.jstrokecerebrovasdis.2017.11.031 PMid:29276014 |
||||
| 27. Pekna M, Pekny M, Nilsson M. Modulation of neural plasticity as a basis for stroke rehabilitation. Stroke. 2012;43(10):2819-28. https://doi.org/10.1161/STROKEAHA.112.654228 PMid:22923444 |
||||
| 28. Zittel S, Weiller C, Liepert J. Citalopram improves dexterity in chronic stroke patients. Neurorehabilitation and neural repair. 2008;22(3):311-4. https://doi.org/10.1177/1545968307312173 PMid:18219053 |
||||
| 29. Organization WH. WHO STEPS Stroke Manual: the WHO STEPwise approach to stroke surveillance. Geneva. World Health Organization. 2006;11. | ||||
| 30. Longo DL, Jameson JL, Kaspe D. Harrison's Principles of Internal Medicine: Volume 2: Macgraw-Hill; 2011. | ||||
| 31. Mikami K, Jorge RE, Adams Jr HP, Davis PH, Leira EC, Jang M, et al. Effect of antidepressants on the course of disability following stroke. The American journal of geriatric psychiatry. 2011;19(12):1007-15. https://doi.org/10.1097/JGP.0b013e31821181b0 PMid:21358384 PMCid:PMC3565535 |
||||
| 32. Selim MH, Molina CA. Poststroke treatment with selective serotonin reuptake inhibitors: a journey from sadness to motor recovery. Stroke. 2012;43(11):3154-5. https://doi.org/10.1161/STROKEAHA.112.657635 PMid:23065004 |
||||
| 33. Marshall RS. Should every patient with stroke be on selective serotonin reuptake inhibitors? No. Stroke. 2012;43(11):3152-3. https://doi.org/10.1161/STROKEAHA.112.657627 PMid:23065003 |
||||
| 34. Hamidi R, Fekrizadeh Z, Azadbakht M, Garmaroudi G, Taheri Tanjani P, Fathizadeh S, et al. Validity and reliability Beck Depression Inventory-II among the Iranian elderly population. Journal of Sabzevar University of Medical Sciences. 2015;22(1):189-98. | ||||
| 35. Toluee Achacheluee S, Rahnama L, Karimi N, Abdollahi I, Jaberzadeh S, Arslan SA. The test-retest reliability and minimal detectable change of the fugl-meyer assessment of the upper extremity and 9-hole pegboard test in individuals with subacute stroke. Research in Rehabilitation Sciences. 2016;5(4):225-30. https://doi.org/10.15412/J.PTJ.07050406 |
||||
| 36. Mead GE, Legg L, Tilney R, Hsieh CF, Wu S, Lundström E, et al. Fluoxetine for stroke recovery: Meta-analysis of randomized controlled trials. International Journal of Stroke. 2020;15(4):365-76. https://doi.org/10.1177/1747493019879655 PMid:31619137 |
||||
| 37. Marquez-Romero JM, Arauz A, Ruiz-Sandoval JL, Cruz-Estrada Edl, Huerta-Franco MR, Aguayo-Leytte G, et al. Fluoxetine for motor recovery after acute intracerebral hemorrhage (FMRICH): study protocol for a randomized, double-blind, placebo-controlled, multicenter trial. Trials. 2013;14(1):1-7. https://doi.org/10.1186/1745-6215-14-77 PMid:23510124 PMCid:PMC3652770 |
||||
| 38. Marquez-Romero JM, Reyes-Martínez M, Huerta-Franco MR, Ruiz-Franco A, Silos H, Arauz A. Fluoxetine for motor recovery after acute intracerebral hemorrhage, the FMRICH trial. Clinical Neurology and Neurosurgery. 2020;190:105656. https://doi.org/10.1016/j.clineuro.2019.105656 PMid:31896491 |
||||
| 39. Liberati A, Altman DG, Tetzlaff J, Mulrow C, Gøtzsche PC, Ioannidis JP, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. Journal of clinical epidemiology. 2009;62(10):e1-e34. https://doi.org/10.1016/j.jclinepi.2009.06.006 PMid:19631507 |
||||
| 40. Powers WJ, Rabinstein AA, Ackerson T, Adeoye OM, Bambakidis NC, Becker K, et al. 2018 guidelines for the early management of patients with acute ischemic stroke: a guideline for healthcare professionals from the American Heart Association/American Stroke Association. stroke. 2018;49(3):e46-e99. https://doi.org/10.1161/STR.0000000000000158 PMid:29367334 |
||||
| 41. Acler M, Robol E, Fiaschi A, Manganotti P. A double blind placebo RCT to investigate the effects of serotonergic modulation on brain excitability and motor recovery in stroke patients. Journal of neurology. 2009;256:1152-8. https://doi.org/10.1007/s00415-009-5093-7 PMid:19306038 |
||||
| 42. Uyttenboogaart M, Stewart RE, Vroomen PC, De Keyser J, Luijckx G-J. Optimizing cutoff scores for the Barthel index and the modified Rankin scale for defining outcome in acute stroke trials. Stroke. 2005;36(9):1984-7. https://doi.org/10.1161/01.STR.0000177872.87960.61 PMid:16081854 |
||||
| 43. Brott T, Adams Jr HP, Olinger CP, Marler JR, Barsan WG, Biller J, et al. Measurements of acute cerebral infarction: a clinical examination scale. Stroke. 1989;20(7):864-70. https://doi.org/10.1161/01.STR.20.7.871 https://doi.org/10.1161/01.STR.20.7.864 PMid:2749846 |
||||
| 44. McCann SK, Irvine C, Mead GE, Sena ES, Currie GL, Egan KE, et al. Efficacy of antidepressants in animal models of ischemic stroke: a systematic review and meta-analysis. Stroke. 2014;45(10):3055-63. https://doi.org/10.1161/STROKEAHA.114.006304 PMid:25184357 |
||||
| 45. Santarelli L, Saxe M, Gross C, Surget A, Battaglia F, Dulawa S, et al. Requirement of hippocampal neurogenesis for the behavioral effects of antidepressants. science. 2003;301(5634):805-9. https://doi.org/10.1126/science.1083328 PMid:12907793 |
||||
| 46. Taupin P. Adult neurogenesis, neuroinflammation and therapeutic potential of adult neural stem cells. International journal of medical sciences. 2008;5(3):127. https://doi.org/10.7150/ijms.5.127 PMid:18566676 PMCid:PMC2424180 |
||||
| 47. Wiltrout C, Lang B, Yan Y, Dempsey RJ, Vemuganti R. Repairing brain after stroke: a review on post-ischemic neurogenesis. Neurochemistry international. 2007;50(7-8):1028-41. https://doi.org/10.1016/j.neuint.2007.04.011 PMid:17531349 |
||||
| 48. Dempsey RJ, Sailor KA, Bowen KK, Türeyen K, Vemuganti R. Stroke‐induced progenitor cell proliferation in adult spontaneously hypertensive rat brain: effect of exogenous IGF‐1 and GDNF. Journal of neurochemistry. 2003;87(3):586-97. https://doi.org/10.1046/j.1471-4159.2003.02022.x PMid:14535942 |
||||
| 49. Lang UE, Jockers-Scherübl M, Hellweg R. State of the art of the neurotrophin hypothesis in psychiatric disorders: implications and limitations. Journal of neural transmission. 2004;111(3):387-411. https://doi.org/10.1007/s00702-003-0100-0 PMid:14991461 |
||||
| 50. Mead GE, Hsieh CF, Lee R, Kutlubaev MA, Claxton A, Hankey GJ, et al. Selective serotonin reuptake inhibitors (SSRIs) for stroke recovery. Cochrane Database of Systematic Reviews. 2012(11). https://doi.org/10.1002/14651858.CD009286.pub2 PMCid:PMC6465036 |
||||
| 51. Dirnagl U, Iadecola C, Moskowitz MA. Pathobiology of ischaemic stroke: an integrated view. Trends in neurosciences. 1999;22(9):391-7. https://doi.org/10.1016/S0166-2236(99)01401-0 PMid:10441299 |
||||
| 52. Kirino T. Delayed neuronal death. Neuropathology. 2000;20:95-7. https://doi.org/10.1046/j.1440-1789.2000.00306.x PMid:11037198 |
||||
| 53. Lim CM, Kim SW, Park JY, Kim C, Yoon SH, Lee JK. Fluoxetine affords robust neuroprotection in the postischemic brain via its anti‐inflammatory effect. Journal of neuroscience research. 2009;87(4):1037-45. https://doi.org/10.1002/jnr.21899 PMid:18855941 |
||||
| 54. Ozaki H, Yu A, Della N, Ozaki K, Luna JD, Yamada H, et al. Hypoxia inducible factor-1alpha is increased in ischemic retina: temporal and spatial correlation with VEGF expression. Investigative ophthalmology & visual science. 1999;40(1):182-9. | ||||
| 55. Shin TK, Kang MS, Lee HY, Seo MS, Kim SG, Kim CD, et al. Fluoxetine and sertraline attenuate postischemic brain injury in mice. The Korean Journal of Physiology & Pharmacology. 2009;13(3):257-63. https://doi.org/10.4196/kjpp.2009.13.3.257 PMid:19885045 PMCid:PMC2766739 |
||||
| 56. Russo-Neustadt A, Chen M. Brain-derived neurotrophic factor and antidepressant activity. Current pharmaceutical design. 2005;11(12):1495-510. https://doi.org/10.2174/1381612053764788 PMid:15892658 |
||||
| 57. Balu DT, Hoshaw BA, Malberg JE, Rosenzweig-Lipson S, Schechter LE, Lucki I. Differential regulation of central BDNF protein levels by antidepressant and non-antidepressant drug treatments. Brain research. 2008;1211:37-43. https://doi.org/10.1016/j.brainres.2008.03.023 PMid:18433734 PMCid:PMC2394727 |
||||
| 58. Lindmark B. Evaluation of functional capacity after stroke with special emphasis on motor function and activities of daily living. Scandinavian Journal of Rehabilitation Medicine. 1988. | ||||
| 59. Li WL, Yu SP, Ogle ME, Ding XS, Wei L. Enhanced neurogenesis and cell migration following focal ischemia and peripheral stimulation in mice. Developmental neurobiology. 2008;68(13):1474-86. https://doi.org/10.1002/dneu.20674 PMid:18777565 PMCid:PMC2756802 |
||||
| 60. Espinera AR, Ogle ME, Gu X, Wei L. Citalopram enhances neurovascular regeneration and sensorimotor functional recovery after ischemic stroke in mice. Neuroscience. 2013;247:1-11. https://doi.org/10.1016/j.neuroscience.2013.04.011 PMid:23590907 PMCid:PMC3916088 |
||||
| 61. Wiart L, Petit H, Joseph P, Mazaux J, Barat M. Fluoxetine in early poststroke depression: a double-blind placebo-controlled study. stroke. 2000;31(8):1829-32. https://doi.org/10.1161/01.STR.31.8.1829 PMid:10926942 |
||||
| 62. Gainotti G, Antonucci G, Marra C, Paolucci S. Relation between depression after stroke, antidepressant therapy, and functional recovery. Journal of Neurology, Neurosurgery & Psychiatry. 2001;71(2):258-61. https://doi.org/10.1136/jnnp.71.2.258 PMid:11459907 PMCid:PMC1737529 |
||||
| 63. Jorge RE, Robinson RG, Arndt S, Starkstein S. Mortality and poststroke depression: a placebo-controlled trial of antidepressants. American Journal of Psychiatry. 2003;160(10):1823-9. https://doi.org/10.1176/appi.ajp.160.10.1823 PMid:14514497 |
||||
| 64. Pedersen OL, Kragh-Sørensen P, Bjerre M, Overø KF, Gram L. Citalopram, a selective serotonin reuptake inhibitor: clinical antidepressive and long-term effect-a phase II study. Psychopharmacology. 1982;77(3):199-204. https://doi.org/10.1007/BF00464566 PMid:6812140 |
||||

| Article View | 763 |
| PDF Download | 332 |