Document Type : Review Article
Keywords
Subjects
Introduction
COVID-19 is a mild to moderate and self-limited illness in most cases and it is caused by severe acute respiratory syndrome coronavirus-2 (SARS-COV-2), a novel coronavirus (1, 2). Currently, more than 755 million confirmed cases are reported by WHO worldwide (3). However, most of the studies have focused on respiratory symptoms and neurological manifestations have been increasingly reported (4, 5). Some previous studies reported acute ischemic stroke in patients infected by SARS-COV-2 (6). Qin C et al demonstrated a mechanism through cytokines involved in the inflammatory procedures which can accelerate endothelial damage and thus the condition of hypercoagulation in the vessels (7). Moreover, angiotensin-converting enzyme-2 (ACE-2) as a binding site of SARS-CoV-2 is shown to have an effective role in the constriction and hypertension of the brain vessels, which in turn increase the risk of ischemic stroke in patients with COIVD-19 (8, 9).
Some other studies have reported acute disseminated encephalomyelitis (ADEM) as a neuroimaging manifestation of COVID-19 patients (10, 11). ADEM is a monophasic demyelinating disease that is commonly caused by upper respiratory tract infections such as COVID-19 (12). Due to the lack of appropriate biomarkers this disease is diagnosed based on neuroimaging techniques such as MRI (13). Moreover, some studies have investigated olfactory sensory changes in patients with COVID-19 demonstrating dysfunction of olfactory sensory nerve endings (14, 15). Considering the mechanism of retrograde transmission of this virus through olfactory nerves, some studies have hypothesized that the piriform cortex as an important sensory cortical area of the olfactory brain network can be affected by SARS‐CoV‐2 in infected patients (16, 17). Metabolic changes in the central nervous system (CNS) after COVID-19 are also reported in recent studies (18). Some of them by using the 18F-FDG PET method have revealed decreased metabolism of limbic and paralimbic regions as well as the cerebellum (19). Some also have demonstrated a depletion of metabolism in the right parahippocampal gyrus and thalamus which in turn are associated with the poor performance of the Montreal Cognitive Assessment (MoCA) in COVID-19 patients (20).
In addition to the aforementioned neuroimaging deficits, microstructural and structural neuroimaging findings have also been observed in COVID-19 patients (21, 22). These findings include changes in white matter (WM) integrity, reductions in gray matter (GM) volume, and abnormalities in cortical thickness. These structural changes are thought to be related to the neuroinflammatory response triggered by the virus, which can lead to neurodegeneration and neuronal death (23, 24). Moreover, recent studies have reported the presence of microhemorrhages and microinfarcts in the brains of COVID-19 patients, which may contribute to the neurological complications observed in some cases (25). These findings highlight the need for increased attention to the neurological consequences of COVID-19 and the importance of incorporating neuroimaging into the diagnostic and treatment protocols for affected patients. Proper identification and management of neurological complications in COVID-19 patients can improve their overall prognosis and quality of life.
The aim of our systematic review study is to evaluate the current state of knowledge regarding neuroimaging findings after COVID-19 by focusing on longitudinal studies. By limiting our review to this type of study design, we aimed to provide a more comprehensive and detailed picture of the long-term effects of COVID-19 on the brain. We believe that our review will contribute to a better understanding of the neurological complications associated with COVID-19 and help guide future research and clinical practice.
Methods and materials
The present study was conducted following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses “PRISMA” statement (26).
Search strategy
Three electronic databases (PubMed, Scopus, and Web of Science) were searched for relevant studies. The following terms were used in our search strategy: “COVID-19” OR “coronavirus” OR “sars-cov-2” OR “Severe Acute Respiratory Syndrome Coronavirus 2” OR “2019-nCoV” AND “brain” AND “DTI” OR “diffusion tensor imaging” OR “microstructure” OR “anisotropy” OR “Diffusivity” OR “functional magnetic resonance imaging” OR “functional MRI” OR “fMRI” OR “rsfMRI” OR “resting-state fMRI” OR “Brain mapping” OR “Structural MRI” OR “voxel-based morphometry” OR “gray matter” OR “white matter” OR “MRI” OR “magnetic resonance imaging”. Additionally, we manually searched the reference list of review studies for relevant papers.
Eligibility criteria
We included studies that investigated brain imaging findings in patients with COVID-19. The eligibility criteria for the published paper: 1) confirmed COVID-19 diagnosis using PCR or serum antibody; 2) available neuroimaging findings at two different times (longitudinal design); 3) reporting sufficient details on neuroimaging findings. The following studies were excluded: 1) Review studies; 2) case reports and case series; 3) Editorials; 4) Studies with cross-sectional design; 5) Non-English papers.
Study selection
Two investigators (S.F, and M.A) independently screened titles and abstracts in the first step and excluded irrelevant studies. Then, the same investigators reviewed the full text of remained articles and selected papers that met our eligibility criteria. Any disagreements were resolved by consulting with the third investigator (F.N).
Data extraction
The same researchers (S.F, and M.A) obtained the following data from included studies using a pre-designed data sheet: Study’s demographics, follow-up duration, neuroimaging modality, number of patients, mean age, gender, inclusion criteria for the patients, clinical status of the patients, number of critically ill patients, type of neuroimaging analysis, main neuroimaging findings, and detailed neuroimaging findings.
Quality assessments
The quality of included studies was assessed by two investigators (S.F, and M.A) using the Newcastle-Ottawa scale (NOS) in several aspects (27).
Results
Study selection
Our literature search and manual addition yielded 3674 studies (Figure 1). After duplicate removal, 2691 papers underwent the screening process. First, 2583 studies were excluded after the title and abstract review. Finally, 10 studies were included in our qualitative synthesis (28-37).
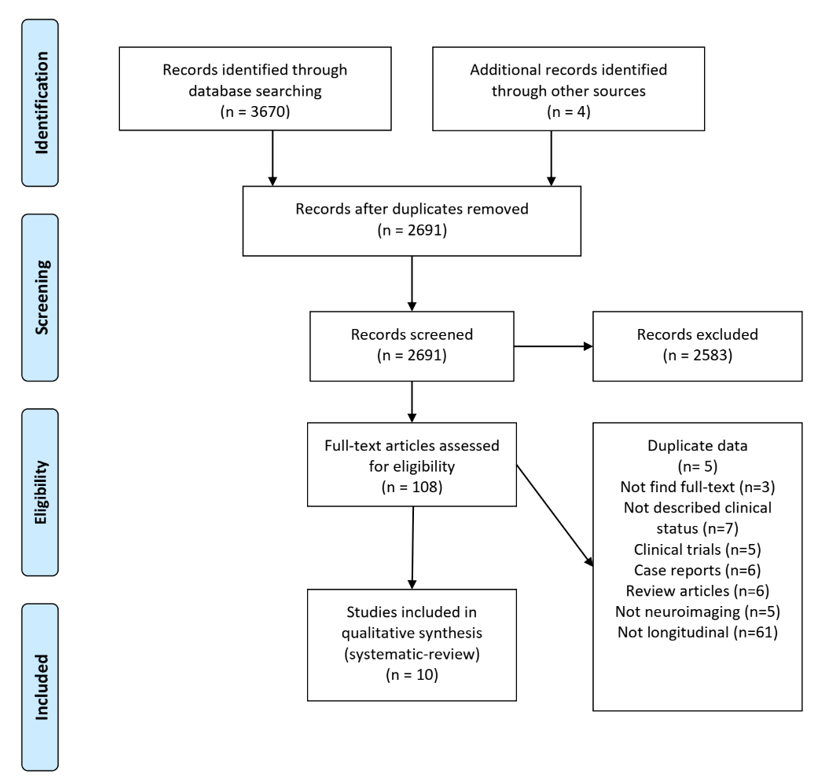
Figure 1. PRISMA flow diagram depicting the flow of information through the different phases of a systematic review.
Study characteristics
The detailed demographic of included studies is presented in Table 1. Among included studies, six had cohort design (28, 30, 32, 33, 35, 37), three were observational (29, 34, 36) and one was case-control (31). Brain MRI was the only imaging modality in seven studies (28-32, 36, 37), whereas one used only FDG-PET (34), one used CT/MRI (33), and one used CT/MRI/FDG-PET (35). Overall, 1212 subjects (women=596) with mean age ranged between 27.4 to 69.4. All patients with COVID-19 had confirmed diagnoses using PCR or serum antibodies (Table 2). The quality assessment of included studies detailed in Supplementary 1 There were no concerns regarding the quality of studies and risk of bias.
|
Table1. Demographic characteristics of the included studies |
||||||||||
|
Author |
Country |
study design |
Multi-center(yes or no) |
Study period |
Follow-up duration |
Neuroimaging modality |
Image methods |
Number of patients with Neuroimaging data |
Mean age |
sex (Male) |
|
Agarwal et al. 2021 |
US |
Retrospective cohort |
No |
March 1, 2020 to June 30, 2020 |
49 days |
MRI |
Susceptibility weighted imaging (SWI), T2*-weighted gradient-recalled echo |
21 |
60 |
0.86 |
|
Hellgren et al. 2021 |
Sweden |
Ambidirectional observational cohort |
No |
March 1, 2020 to March 31, 2020 |
4 months |
MRI |
T2-FLAIR, T2-FSE, T1-FSE, DWI, T1-GRE, SWI |
35 (6 had previous MRI in the acute phase) |
59 (Median) |
0.8 |
|
Kas et al. 2021 |
France |
Prospective obervational |
No |
March to June 2020 |
6 months |
FDG-PET |
NR |
7 |
63 (Median) |
0.57 |
|
Salomon et al. 2021 |
Israel |
Observational |
No |
May 1, 2020 to July 29, 2020 |
67 - 1460 days |
MRI |
T1w anatomical scan with MPRAGE |
Test group: 50, Control group: 50 |
Test: 30.1, Control: 27.4 |
Test: 60%, Control: 54% |
|
Ammar et al. 2021 |
France |
Prospective obervational |
Yes |
March to May 2020 |
6 months |
MRI |
3D-FLAIR-CUBE, 3D-T2-FIESTA |
11 |
41.5 |
0.363 |
|
Del Brutto et al. 2022 |
Ecuador |
Prospective cohort |
No |
NR |
1.4 years |
MRI |
T2-weighted sequence |
93 (26 in group 1 and 67 in group 2) |
69.4 |
0.4 |
|
Douaud et al. 2022 |
UK |
Case-control |
Yes |
February 2021 to May 31, 2021 |
141 days |
MRI |
T1-FLAIR, T2-FLAIR, SWI, diffusion MRI, resting fMRI |
785 (401 cases and 384 controls) |
Scan 1: 58.9 (case group), 60.2 (control group). Scan 2: 62.1 (case group), 63.3 (control group) |
42.9% (case), 42.7% (control) |
|
Ippolito et al. 2022 |
Germany |
Ambidirectional observational cohort |
No |
February 1, 2020 to June 30, 2021 |
NR |
CT, MRI |
T1W spin echo, T2W turbo spin echo, time-of-flight MR-angiography, DWI |
64 (13 patients with follow-up imaging) |
61 |
0.86 |
|
Lersy et al. 2022 |
France |
Prospective observational |
No |
March 1, 2020 to May 31, 2020 |
3 or 6 months |
MRI, FDG-PET/CT |
T1W spin-echo, DWI, SWI, perfusion-weighted, 2D or 3D FLAIR |
31 |
61 |
0.74 |
|
Tian et al. 2022 |
China |
Prospective cohort |
No |
March 2020 to January 2021 |
10 months |
MRI |
3D-T1W, 3D-pcASL, DTI |
65 (13 in mild COVID-19 group, 21 in severe COVID-19 group, and 31 controls) |
Mild group: 58.1, Severe group: 62.7, Control group: 60.5 |
Mild group: 46.1%, Severe group: 47.6%, Control group: 58.0% |
|
MRI, Magnetic resonance imaging; PET, Positron emission tomography; CT, Computerized tomography; NR, not reported |
||||||||||
Neuroimaging findings
MRI was the most common imaging technique used in nine studies (28-33, 35-37), however, one study used FDG/PET imaging modality as radiological tool (34). Seven studies conducted a volumetric analysis (28-31, 35-37), one used the SPM-based analysis (34), and other two studies used statistical analysis methods based on expert's view (32, 33).
WM alterations
The main outcome of these studies was identifying alteration in WM, reduction in GM thickness, cerebral blood flow alterations, and transient volumetric changes in areas in regions associated with stress and anxiety, and also transient change in olfactory bulb.
Agarwal et.al evaluated serial imaging of 21 patients and found an increase in ventricle size and alterations in WM, specifically in the periventricular area in all patients on both initial and follow-up imagings (28). WM changes in other regions were as follow on both initial and follow-up imagings respectively: juxtacortical (81%, 81%), subcortical (81%, 91%), brainstem (29%, 33%), precentral gyrus (29%, 24%), and cerebellum (19%, 19%). In another study, Hellgern et. al showed presence of multiple WM lesions (71%, n=25) located in the cerebral hemispheres near the grey-WM junction, particularly in the frontal and parietal lobes. Moreover, all the patients who underwent MRI during the acute phase of COVID-19 had acquired multiple new WM lesions when examined at follow-up.
Another study found changes in markers of tissue damage such as diffusion measures in regions functionally connected to the temporal piriform cortex (31). Douaud et. al compared 401 cases with 384 controls and showed significant longitudinal differences in a network of regions that is functionally connected to the piriform cortex, mainly consisting of the anterior cingulate cortex and orbitofrontal cortex, as well as the ventral striatum, amygdala, hippocampus and parahippocampal gyrus.
|
Table2. Clinical characteristics of the included studies |
||||
|
Author |
Number of patients with Neuroimaging data |
Inclusion criteria for patients |
Clinical status of patients |
Number of critically ill patients |
|
Agarwal et al. 2021 |
21 |
Patients diagnosed with COVID-19 via nasopharyngeal swab PCR with multiple brain MRI scans. |
NR |
21 |
|
Hellgren et al. 2021 |
35 (6 had previous MRI in the acute phase) |
Laboratory-diagnosed COVID-19 patients who underwent MRI at follow-up |
NR |
20 |
|
Kas et al. 2021 |
7 |
Hospitalized patients with COVID-19-related encephalopathy |
Severe executive deficit and frontal behavioral changes with apathy (all patients), psychiatric manifestations (5 patients), cerebellar syndrome (2 patients), myoclonus (2 patients), oculomotor disturbances (2 patients). Required mechanical ventilation (3 patients), required nasal oxygen (3 patients) |
NR |
|
Salomon et al. 2021 |
Test group: 50, Control group: 50 |
Particippants scanned before and after pandemic(test) and participants scanned twice before pandemic (control). |
All particioants had no background of neurological disorders, did not show symptoms of COVID-19 infection and were not diagnosed as carriers of the virus. |
NR |
|
Ammar et al. 2021 |
11 |
COVID-19 patients with self reported sudden olfactory dysfunction |
All pateints were initially anosmic. Seasonal allergy (3 patients), septoplasty (2 patients), dysthyroidism (2 patients), hypertension (1 patient), cardiac stent (1 patient), autoimmune disease (1 patient), and endometriosis (1 patient). |
NR |
|
Del Brutto et al. 2022 |
93 (26 in group 1 and 67 in group 2) |
Participants with good sleep quality at baseline, evidence of COVID-19 infection, and MRIs at baseline and follow-up. |
BMI ≥30 kg/m2 (22 patients), hypertension (34 patients), persistant poor sleep quality in group 1, good sleep quality or transient poor sleep quality in group 2 |
NR |
|
Douaud et al. 2022 |
785 (401 cases and 384 controls) |
Participants that have already attended one of the imaging sites, had no incidental findings in their first scans, had high-quality scans from their first imaging visit, had not withdrawn or died, lived within 60km of the clinic, and had a valid email and postal address. Cases were subjects that have been infected with SARS-CoV-2 identified with antigen tests, their primary care data or health records, or two antibody tests. |
Hospitalised (15 patients), critical care unit (2 patients), invasive ventilation (1 patient), Continuous positive airway pressure (1 patient), Non-invasive ventilation (1 patient), unspecified oxygen therapy (1 patient) |
2 |
|
Ippolito et al. 2022 |
64 (13 patients with follow-up imaging) |
Critically ill patients with confirmed diagnosis of COVID-19. |
Pathological arousal levels (41 patients), pathological brain stem function (21 patients), pathological motor responses (2 patients), unilateral neglect and hemiparesis (1 patient), sensorimotor deficits of both legs (1 patient). |
64 |
|
Lersy et al. 2022 |
31 |
COVID-19 patients with neurological symptoms who underwent MRI. |
Pathological wakefulness (14 patients), Delirium (9 patients), Signs of corticospinal tract involvement (6 patients) |
31 |
|
Tian et al. 2022 |
65 (13 in mild COVID-19 group, 21 in severe COVID-19 group, and 31 controls) |
Recovered Covid-19 patients that were 50-70 years old and had no clear neurological manifestations and lesions on MRI and had no history of stroke, head trauma, brain tumors, or epilepsy. |
Hypertension (15% in mild, 52% in severe, 35% in control), Diabetes (15 % in mild, 29% in severe, 6% in control), Corornal heart disease (8% in mild, 14% in severe, 3% in control) |
NR |
|
NR, not reported |
||||
GM alterations
In another study Tian et. al investigated the changes in the brain volume, tractography, and blood flow in recovered COVID-19 patients (37). They reported increased GM thickness in the left limbic areas, right parahippocampus, bilateral frontal cortex, and left temporal-parietal cortex in the mild group after 10 months follow-up. In the severe group, thicker GM in the left limbic areas and left temporal-frontal cortex and GM atrophy was displayed in the right sensorimotor areas and right temporal-parietal cortex after 10 months follow-up. Another study, done by Douaud et.al which was investigated the impact of SARS-CoV-2 infection on brain structure, found a greater reduction in GM thickness and tissue contrast in the orbitofrontal cortex and parahippocampal gyrus, greater changes in markers of tissue damage in regions functionally connected to primary olfactory cortex, and a greater reduction in global brain size in these cases (31). The infected patients also showed on average a greater cognitive decline between the two time points.
|
Table3. Neuroimaging findings |
|||||||
|
Author |
Follow-up duration |
Neuroimaging modality |
Image methods |
Number of patients with Neuroimaging data |
Type of neuroimaging analysis ( |
Main neuroimaging findings |
Detailed neuroimaging findings |
|
Agarwal et al. 2021 |
49 days |
MRI |
Susceptibility weighted imaging (SWI), T2*-weighted gradient-recalled echo imaging (GRE) |
21 |
Volumetric |
Increase in ventricle size, white matter changes |
The median bicaudate index and third ventricular diameter increased, with varying WM changes across patients. Initial and follow-up imaging showed WM changes in various regions, with patients also experiencing conditions like microhemorrhages, strokes, and necrosis or cystic changes in WM. |
|
Hellgren et al. 2021 |
4 months |
MRI |
T2-FLAIR, T2-FSE, T1-FSE, DWI, T1-GRE, SWI |
35 (6 had previous MRI in the acute phase) |
Expert's view |
White matter lesions |
Subcortical white matter lesions near the grey-white matter junction were found in 25 patients, with additional lesions in those with previous MRIs. Seven patients had confluent white matter lesions with a biparietal distribution, and eight showed subcortical abnormalities on the SWI. |
|
Kas et al. 2021 |
6 months |
PET |
NR |
7 |
Glucose metabolism changes |
Hypometabolism in several cerebral networks |
During the acute phase, patients experienced prominent hypometabolism in several brain regions and mild hypermetabolism in the vermis, dentate nucleus, and pons. At follow-up, brain metabolism was almost normal, with mild hypometabolism in a few areas. |
|
Salomon et al. 2021 |
67 - 1460 days |
MRI |
T1w anatomical scan with MPRAGE |
Test group: 50, Control group: 50 |
Volumetric |
Transiet volumetric changes in areas associated with stress and anxiety |
Increased volume in bilateral amygdalae, putamen, and anterior temporal cortices namely the medial part of the anterior temporal lobe, the fusiform gyrus, and the parahippocampal gyrus in test group. |
|
Ammar et al. 2021 |
6 months |
MRI |
3D-FLAIR-CUBE, 3D-T2-FIESTA |
11 |
Volumetric |
Transient change in olfactory bulb |
Five patients had partial olfactory cleft obstruction, three of which were bilateral. Initial increase in olfactory bulb volume and signal intensity was observed, which normalized on follow-up. |
|
Del Brutto et al. 2022 |
1.4 years |
MRI |
T2-weighted sequence |
93 (26 in poor sleep quality group and 67 in good sleep quality group) |
Volumetric |
Enlarged basal ganglia-perivascular spaces |
The study found that persistent poor sleep quality significantly impacts the progression of basal ganglia and perivascular spaces, with 11 subjects in the poor sleep quality group and 9 in the good sleep quality group. |
|
Douaud et al. 2022 |
141 days |
MRI |
T1-FLAIR, T2-FLAIR, SWI, diffusion MRI, resting fMRI |
785 (401 cases and 384 controls) |
Volumetric |
Reduction in grey matter thickness, changes in markers of tissue damage, redcution in global brain size |
Diffusion measures in various brain regions and the ratio of brain volume to total intracranial volume showed significant changes, along with an increase in normalized CSF and right lateral ventricle volumes. There were also reductions in grey matter thickness in several areas. |
|
Ippolito et al. 2022 |
NR |
CT, MRI |
T1W spin echo, T2W turbo spin echo, time-of-flight MR-angiography, DWI |
64 (13 patients with follow-up imaging) |
Expert's view |
acute pathological neuroimaging findings |
The report indicates various brain conditions: severe (n=9) and mild (n=4) intracerebral hemorrhages, acute cerebral infarction in 8 patients (4 of which had secondary intracerebral hemorrhage), and 2 patients had numerous tiny microhemorrhages mainly in the juxtacortical white matter. |
|
Lersy et al. 2022 |
3 or 6 months |
MRI, FDG-PET/CT |
T1W spin-echo, DWI, SWI, perfusion-weighted, 2D or 3D FLAIR |
31 |
Volumetric, perfusion, metabolic |
Alterations of lesions, cerebral blood flow, and metabolism |
The study reports various neurological conditions in subjects including focal leptomeningeal enhancement, diffuse brain microhemorrhages, acute ischemic strokes, suspected cerebral vasculitis, and acute inflammatory demyelinating lesions. Additionally, the evolution of lesions varied, with hypoperfusion and reduced grey matter volume being common, and metabolic changes were observed in the colliculi and temporal and insular regions. |
|
Tian et al. 2022 |
10 months |
MRI |
3D-T1W, 3D-pcASL, DTI |
65 (13 in mild COVID-19 group, 21 in severe COVID-19 group, and 31 controls) |
Volumetric, tractography, cerebral blood flow |
Recovered cortical thickness and hypoperfusion, reduced volume of subcortical nuclei |
The study found varying brain changes in mild and severe groups, including differences in gray matter thickness and atrophy, cerebral blood flow, and volumes of certain brain structures. Additionally, there were changes in white matter tract volumes in both groups, with some areas showing increased volume and others showing decreased volume compared to controls. |
|
MRI, Magnetic resonance imaging; PET, Positron emission tomography; CT, Computerized tomography; NR, not reported |
|||||||
In another study, done by Salmon et. al, they analyzed volumetric changes in 50 individuals who received MRI scans before and after the COVID-19 outbreak and lockdown in Israel (36). Their scans were contrasted with those of 50 control participants who underwent two scans before the pandemic. After the COVID-19 outbreak and lockdown, the test group participants displayed unique volume increases in the bilateral amygdalae, putamen, and anterior temporal cortices. As time passed since the easing of lockdown restrictions, changes in the amygdalae decreased, indicating that the intense experience related to the pandemic caused temporary volume changes in brain areas typically linked to stress and anxiety. In another study, Del Brutto et al found enlarged basal ganglia-perivascular spaces as another morphologic alteration expressed in individuals with long COVID persistent poor sleep quality (30). However, despite the longitudinal design, they were unable to establish a causal link between the continuous presence of poor sleep quality and the advancement of enlarged basal ganglia-perivascular spaces.
Olfactory bulb alteration
Ammar et al. performed a study to seek the neuroimaging characteristics of COVID-19 patients who reported sudden olfactory dysfunction (29). They found a transient change in the olfactory bulb including partial olfactory cleft obstruction (5/11), and bilateral olfactory bulb obstruction (3/11). MR imaging in COVID-19 anosmic patients showed initial increase in signal intensity and volume of olfactory bulbs with a normalization on 6 months-MRI-follow-up whilst 90% of our patients clinically recovered smell. Douaud et al. found notable consequences linked to SARS-CoV-2 infection, mainly involving increased atrophy and tissue harm in cortical regions directly related to the primary olfactory cortex, as well as alterations in overall brain and cerebrospinal fluid volume measurements (31). Longitudinal variation was observed in diffusion measures regions that are functionally connected to the piriform cortex (diffusion index: orientation dispersion), olfactory tubercle (diffusion index: isotropic volume fraction) and anterior olfactory nucleus. However, no differences were seen in the olfactory bulbs or piriform cortex per se.
Blood flow alteration
Cerebral hypoperfusion, hyperperfusion, intracerebral hemorrhage and ischemic stroke and have been reported in several studies as COVID-19 complications. The next study (Ippolito) which involved 64 critically ill patients with a confirmed diagnosis of COVID-19 reported intracerebral hemorrhage (9 severe, 4 mild), acute cerebral infarction (8 patients, 4 with secondary ICH), innumerable, punctuate microhemorrhages that predominantly involved the juxtacortical WM (2 patients) (33). Lersy et. al aimed to find changes in cerebral blood flow of 24 patients who had brain perfusion imaging at different time points (35). Among these 24 patients, 19 (79%) had abnormal brain perfusion on the initial imaging: 16 (66.7%) patients had hypoperfusion and 4 (17%) had hyperperfusion. Overall, 16 (84%) patients showed at least partial normalization of their brain perfusion. Diffuse brain microhemorrhages predominantly happened in the corpus callosum, the subtentorial juxtacortical WM, the internal capsule, the brainstem, the middle cerebellar peduncles, and the cerebellum. Additionally, acute ischemic strokes and suspected cerebral vasculitis were observed in 4 patients. Moreover, Tian et. al reported significant differences regarding extensive lower cerebral blood flow values were observed between severe group at 10 months after discharge
and control groups, especially in bilateral frontal cortices and temporal cortices (37). In another study, Agarwal et al, reported most patients (86%) had microhemorrhages. Other cerebrovascular complications were as follows: ischemic stroke (5/21 patients), cortical ribboning (3 patients), hemorrhagic stroke (1 patient), subarachnoid and intraventricular hemorrhage (1 patient), and pachymeningeal enhancement (1 patient) (28).
Hypometabolism in several cerebral networks
Kas et. al used 18F-FDG-PET/CT imaging and detected prominent hypometabolism of the prefrontal cortex, bilateral insula, and right and left caudate nucleus in the acute phase of COVID-19 (34). Furthermore, at the follow-up brain metabolism returned to almost normal with mild hypometabolism in the rectus/ olfactory gyrus, right insula, anterior cingulate, and right caudate nucleus.
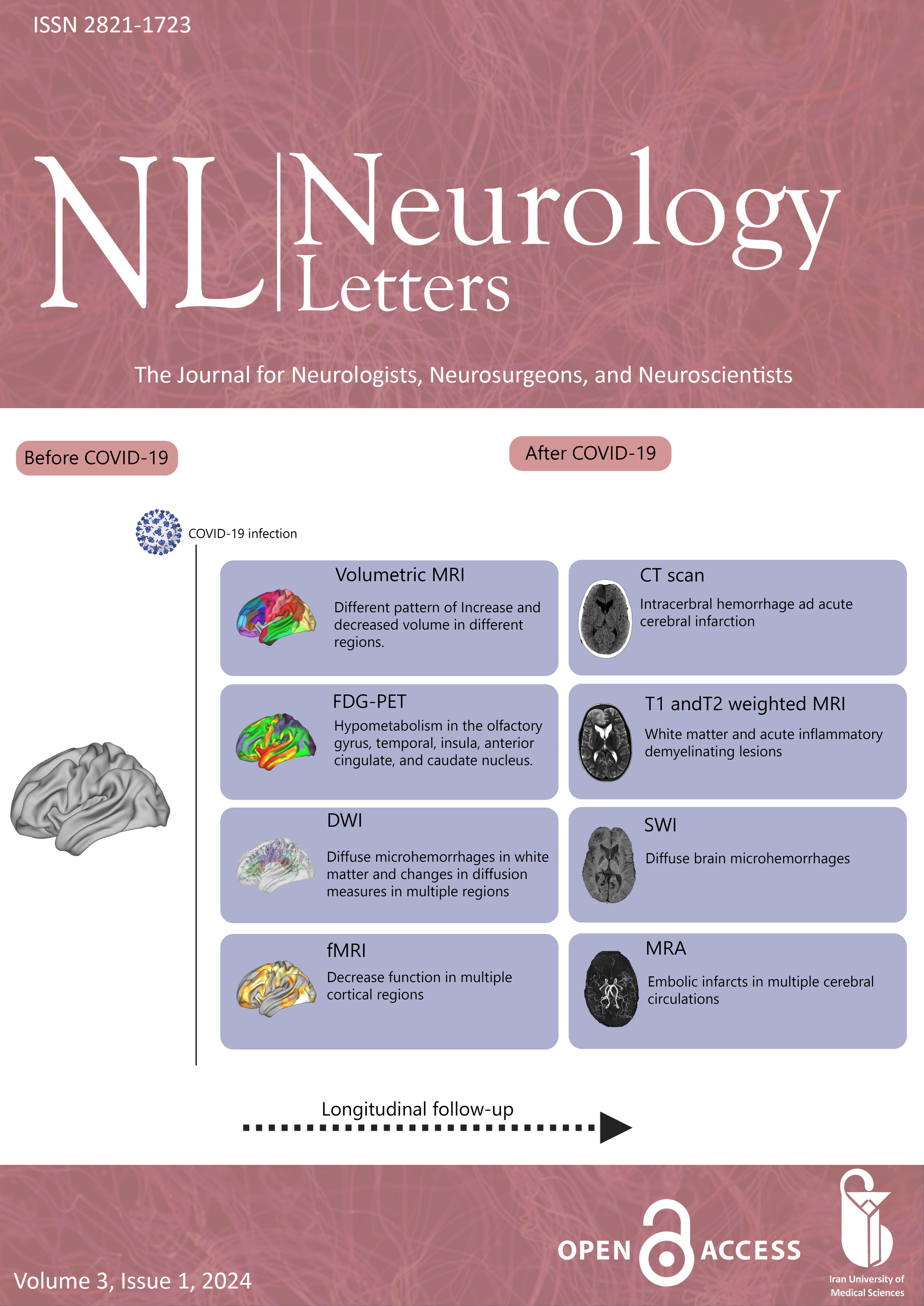
.png)
Figure 2. Overview on longitudinal neuroimaging findings after COVID-19 infection.
Discussion
The aim of the present study was to provide a complete overview of the effect of COVID-19 on brain. This is the first systematic review investigating longitudinal neuroimaging findings of COVID-19 patients.
Our results demonstrated consistent evidence of WM and GM microstructural, metabolism, and blood flow alterations in comparison with healthy controls. The results of this study provide data on neuroimaging alterations in patients suffering from COVID-19 and therefore, may aid radiologists in determining the imaging findings of COVID-19.
Agarwal et al. reported WM alteration across various regions of the brain, indicating a widespread impact of the virus (28). The periventricular area, which is crucial for transmitting nerve signals, was affected in all patients. Also, the changes in the juxtacortical, subcortical, brainstem, precentral gyrus, and cerebellum regions suggest that COVID-19 may disrupt various cognitive and motor functions. The presence of multiple WM lesions, particularly in the frontal and parietal lobes, could potentially affect executive functions and sensory
processing. The fact that new lesions were acquired even during the follow-up period indicates a persistent effect of the COVID-19 on the brain and subsequent cognitive function.
Recent studies indicates that COVID-19 has the potential to affect the WM in the brain, a critical component for cognitive functioning (38). The WM is particularly susceptible to alterations in cerebral blood flow, which can be observed in conjunction with diffuse small vessel dysfunction and has been documented in COVID-19 cases (38). Patients with COVID-19 may experience damage to the WM, resulting in cognitive deficits such as memory loss, short-term memory impairments, attention problems, difficulties with abstraction, long-term memory issues, visuoperception challenges, and disturbances in spatial and temporal orientation (38, 39). However, a study conducted in 2022 observed no substantial decline in cognitive function among individuals who had recovered from COVID-19 after one year of follow-up (40).
GM alterations were also significant. The increased thickness in the left limbic areas, right parahippocampus, bilateral frontal cortex, and left temporal-parietal cortex could be a compensatory response to the virus's impact (37). However, the GM atrophy in the right sensorimotor areas and right temporal-parietal cortex suggests a potential long-term impact on sensory processing and motor functions. The greater reduction in GM thickness and tissue contrast in the orbitofrontal cortex and parahippocampal gyrus, regions associated with cognitive and emotional processing, could explain the cognitive decline observed in some patients.
The transient changes in the olfactory bulb, including partial olfactory cleft obstruction and bilateral olfactory bulb obstruction, provide a explanation for the sudden olfactory dysfunction reported by many COVID-19 patients (29). The normalization of these changes over time aligns with the clinical recovery of smell, suggesting a direct impact of the virus on the olfactory system.
The alterations in cerebral blood flow, including both hypoperfusion and hyperperfusion, could potentially lead to various cerebrovascular complications (28, 33-35). The occurrence of intracerebral hemorrhage, ischemic stroke, and microhemorrhages indicates a significant impact of the COVID-19 on the cerebrovascular system. The extensive lower cerebral blood flow values observed in severe cases suggest a potential long-term impact on cerebral perfusion (35). While most of changes were mostly normalized in the follow-up period, the persistent mild hypometabolism in some regions indicates a potential long-term effect which should be considered in patients recovered from COVID-19.
The pathophysiology underlying the correlation between neuroinflammation induced by COVID-19 and brain alterations, including WMH, olfactory bulb changes, lesions, and hemorrhages, remains an active area of investigation (41-46). Nevertheless, several molecular and cellular mechanisms contributing to the neurological complications of SARS-CoV-2 have been elucidated (42). Among the pathophysiological processes associated with COVID-19-induced neuroinflammation and neuroimaging changes, the infection of neurons by SARS-CoV-2, leading to neuroinflammation, is noteworthy (42). Furthermore, COVID-19 has been implicated in the induction of neuroinflammation and the subsequent loss of hippocampal neurogenesis (44). Also, systemic infection has been observed to activate glial cells, thereby modulating neuroinflammatory responses. This suggests that the infiltration of immune cells and pro-inflammatory mediators into the CNS via the BBB may play a role in glial activation post-COVID-19 (42). Furthermore, the entry of SARS-CoV-2 into the brain parenchyma may result in damage and loss of brain neurons and endothelial cells, thereby induces COVID-19-related neurological symptoms (43). It should be mentioned that vascular risk factors across various age groups appear to augment susceptibility to severe COVID-19 infection. Moreover, clinically evident or subclinical age-related vascular and degenerative diseases in older individuals may exacerbate this risk. The outcomes are likely influenced by acute ischemic lesions and hemorrhages, which are the most prevalent brain findings associated with severe COVID-19 (41).
Results of longitudinal studies revealed that COVID-19 effect on brain returned to normal most of the time. However, several changes remained after recovery, which might be responsible for cognitive impairment and various neurological and psychiatric symptoms. These findings underscore the need for comprehensive neurological assessment and follow-up in COVID-19 patients.
Limitations and future directions
Several limitations must be acknowledged. First, there was considerable heterogeneity in the study design, sample size, and imaging methods of the included studies, which in turn may have caused some variability in the reported results. Second, most of the studies included in this systematic review were observational studies and there should be more longitudinal studies with larger sample sizes to confirm these findings and assess disease progression over time. Third, there was another drawback to our study and it was the varieties in the follow-up durations which may disturb the results. Furthermore, the inclusion criteria of the studies included were heterogenous and it can be taken into consideration for further studies. The type of neuro-imaging analysis was overall volumetric; however, in two studies expert’s view and in another one glucose metabolism changes were used which may affect the results.
Conclusion
In conclusion, our systematic review provides evidence of widespread microstructural, metabolism, and blood flow alterations in patients afflicted with COVID-19. The longitudinal nature of the included studies highlights the importance of ongoing monitoring and follow-up imaging in patients after COVID-19 infection. The observed microstructural changes may have implications for cognitive function and neurological outcomes, underscoring the need for multidisciplinary care in the management of COVID-19 patients. Radiologists and other healthcare providers should remain vigilant about these findings and consider targeted interventions to mitigate potential long-term effects. Overall, this systematic review provides valuable insights into the neuroimaging manifestations of COVID-19 and offers important implications for clinical practice and future research directions and may have a crucial role in the development of novel therapeutic strategies targeting the specific brain regions affected by this virus.
Deceleration
Funding
We do not have any financial support for this study.
Conflict of interest
The authors declare no conflict of interest regarding the publication of this paper.
Ethical approval
Not applicable
Availability of data and material
The datasets analyzed during the current study are available upon request with no restriction.
Consent for publication
This manuscript has been approved for publication by all authors.
| 1. Garg RK, Paliwal VK, Malhotra HS, Sharma PK. Neuroimaging Patterns in Patients with COVID-19-Associated Neurological Complications: A Review. Neurol India. 2021;69(2):260-71. https://doi.org/10.4103/0028-3886.314531 PMid:33904434 |
||||
| 2. de Paula JJ, Paiva R, Souza-Silva NG, Rosa DV, Duran FLS, Coimbra RS, et al. Selective visuoconstructional impairment following mild COVID-19 with inflammatory and neuroimaging correlation findings. Mol Psychiatry. 2023;28(2):553-63. https://doi.org/10.1038/s41380-022-01632-5 PMid:35701598 PMCid:PMC9196149 |
||||
| 3. Nabizadeh F, Seyedalhosseini Z, Balabandian M, Reza Rostami M. Psychological outcomes of the COVID-19 pandemic in patients with Parkinson's disease: A systematic review. Journal of Clinical Neuroscience. 2022;102:101-8. https://doi.org/10.1016/j.jocn.2022.06.017 PMid:35777112 PMCid:PMC9237130 |
||||
| 4. Mao L, Jin H, Wang M, Hu Y, Chen S, He Q, et al. Neurologic Manifestations of Hospitalized Patients With Coronavirus Disease 2019 in Wuhan, China. JAMA Neurol. 2020;77(6):683-90. https://doi.org/10.1001/jamaneurol.2020.1127 PMid:32275288 PMCid:PMC7149362 |
||||
| 5. Helms J, Kremer S, Merdji H, Clere-Jehl R, Schenck M, Kummerlen C, et al. Neurologic Features in Severe SARS-CoV-2 Infection. N Engl J Med. 2020;382(23):2268-70. https://doi.org/10.1056/NEJMc2008597 PMid:32294339 PMCid:PMC7179967 |
||||
| 6. Goldberg MF, Goldberg MF, Cerejo R, Tayal AH. Cerebrovascular Disease in COVID-19. AJNR Am J Neuroradiol. 2020;41(7):1170-2. https://doi.org/10.3174/ajnr.A6588 PMid:32409316 PMCid:PMC7357639 |
||||
| 7. Qin C, Zhou L, Hu Z, Zhang S, Yang S, Tao Y, et al. Dysregulation of Immune Response in Patients With Coronavirus 2019 (COVID-19) in Wuhan, China. Clin Infect Dis. 2020;71(15):762-8. https://doi.org/10.1093/cid/ciaa248 PMid:32161940 PMCid:PMC7108125 |
||||
| 8. Fraga-Silva RA, Da Silva DG, Montecucco F, Mach F, Stergiopulos N, da Silva RF, et al. The angiotensin-converting enzyme 2/angiotensin-(1-7)/Mas receptor axis: a potential target for treating thrombotic diseases. Thromb Haemost. 2012;108(6):1089-96. https://doi.org/10.1160/TH12-06-0396 PMid:23093373 |
||||
| 9. Xia H, Sriramula S, Chhabra KH, Lazartigues E. Brain angiotensin-converting enzyme type 2 shedding contributes to the development of neurogenic hypertension. Circ Res. 2013;113(9):1087-96. https://doi.org/10.1161/CIRCRESAHA.113.301811 PMid:24014829 PMCid:PMC4479408 |
||||
| 10. Reichard RR, Kashani KB, Boire NA, Constantopoulos E, Guo Y, Lucchinetti CF. Neuropathology of COVID-19: a spectrum of vascular and acute disseminated encephalomyelitis (ADEM)-like pathology. Acta Neuropathol. 2020;140(1):1-6. https://doi.org/10.1007/s00401-020-02166-2 PMid:32449057 PMCid:PMC7245994 |
||||
| 11. Nabizadeh F, Noori M, Rahmani S, Hosseini H. Acute disseminated encephalomyelitis (ADEM) following COVID-19 vaccination: A systematic review. Journal of Clinical Neuroscience. 2023;111:57-70. https://doi.org/10.1016/j.jocn.2023.03.008 PMid:36963124 PMCid:PMC10030273 |
||||
| 12. Pohl D, Alper G, Van Haren K, Kornberg AJ, Lucchinetti CF, Tenembaum S, et al. Acute disseminated encephalomyelitis: Updates on an inflammatory CNS syndrome. Neurology. 2016;87(9 Suppl 2):S38-45. https://doi.org/10.1212/WNL.0000000000002825 |
||||
| 13. Manzano GS, McEntire CRS, Martinez-Lage M, Mateen FJ, Hutto SK. Acute Disseminated Encephalomyelitis and Acute Hemorrhagic Leukoencephalitis Following COVID-19: Systematic Review and Meta-synthesis. Neurol Neuroimmunol Neuroinflamm. 2021;8(6). https://doi.org/10.1212/NXI.0000000000001080 PMid:34452974 PMCid:PMC8404207 |
||||
| 14. Meinhardt J, Radke J, Dittmayer C, Franz J, Thomas C, Mothes R, et al. Olfactory transmucosal SARS-CoV-2 invasion as a port of central nervous system entry in individuals with COVID-19. Nat Neurosci. 2021;24(2):168-75. https://doi.org/10.1038/s41593-020-00758-5 PMid:33257876 |
||||
| 15. Sedaghat AR, Gengler I, Speth MM. Olfactory Dysfunction: A Highly Prevalent Symptom of COVID-19 With Public Health Significance. Otolaryngol Head Neck Surg. 2020;163(1):12-5. https://doi.org/10.1177/0194599820926464 PMid:32366160 |
||||
| 16. Esposito F, Cirillo M, De Micco R, Caiazzo G, Siciliano M, Russo AG, et al. Olfactory loss and brain connectivity after COVID-19. Hum Brain Mapp. 2022;43(5):1548-60. https://doi.org/10.1002/hbm.25741 PMid:35083823 PMCid:PMC8886650 |
||||
| 17. Roesch MR, Stalnaker TA, Schoenbaum G. Associative encoding in anterior piriform cortex versus orbitofrontal cortex during odor discrimination and reversal learning. Cereb Cortex. 2007;17(3):643-52. https://doi.org/10.1093/cercor/bhk009 PMid:16699083 PMCid:PMC2396586 |
||||
| 18. Nabizadeh F, Pirahesh K, Sodeifian F, Hashemi SM, Balabandian M, Rezaeimanesh N, et al. Central nervous system autoimmune diseases associated with COVID-19: Comprehensive review. Neurology Letters. 2022;1(2):69-77. https://doi.org/10.52547/nl.1.2.69 |
||||
| 19. Guedj E, Campion JY, Dudouet P, Kaphan E, Bregeon F, Tissot-Dupont H, et al. (18)F-FDG brain PET hypometabolism in patients with long COVID. Eur J Nucl Med Mol Imaging. 2021;48(9):2823-33. https://doi.org/10.1007/s00259-021-05215-4 PMid:33501506 PMCid:PMC7837643 |
||||
| 20. Blazhenets G, Schroeter N, Bormann T, Thurow J, Wagner D, Frings L, et al. Slow but Evident Recovery from Neocortical Dysfunction and Cognitive Impairment in a Series of Chronic COVID-19 Patients. J Nucl Med. 2021;62(7):910-5. https://doi.org/10.2967/jnumed.121.262128 PMid:33789937 PMCid:PMC8882885 |
||||
| 21. Roy-Gash F, De Mesmay M, Devys JM, Vespignani H, Blanc R, Engrand N. COVID-19-associated acute cerebral venous thrombosis: clinical, CT, MRI and EEG features. Crit Care. 2020;24(1):419. https://doi.org/10.1186/s13054-020-03131-x PMid:32653019 PMCid:PMC7351646 |
||||
| 22. Zhou B, She J, Wang Y, Ma X. A Case of Coronavirus Disease 2019 With Concomitant Acute Cerebral Infarction and Deep Vein Thrombosis. Front Neurol. 2020;11:296. https://doi.org/10.3389/fneur.2020.00296 PMid:32390931 PMCid:PMC7188982 |
||||
| 23. Leira EC, Russman AN, Biller J, Brown DL, Bushnell CD, Caso V, et al. Preserving stroke care during the COVID-19 pandemic: Potential issues and solutions. Neurology. 2020;95(3):124-33. https://doi.org/10.1212/WNL.0000000000009713 PMid:32385186 PMCid:PMC7455350 |
||||
| 24. Wira CR, Goyal M, Southerland AM, Sheth KN, McNair ND, Khosravani H, et al. Pandemic Guidance for Stroke Centers Aiding COVID-19 Treatment Teams. Stroke. 2020;51(8):2587-92. https://doi.org/10.1161/STROKEAHA.120.030749 PMid:32716826 PMCid:PMC7326321 |
||||
| 25. Al-Olama M, Rashid A, Garozzo D. COVID-19-associated meningoencephalitis complicated with intracranial hemorrhage: a case report. Acta Neurochir (Wien). 2020;162(7):1495-9. https://doi.org/10.1007/s00701-020-04402-w PMid:32430637 PMCid:PMC7237227 |
||||
| 26. Liberati A, Altman DG, Tetzlaff J, Mulrow C, Gøtzsche PC, Ioannidis JPA, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: explanation and elaboration. BMJ. 2009;339:b2700. https://doi.org/10.1136/bmj.b2700 PMid:19622552 PMCid:PMC2714672 |
||||
| 27. Wells GA, Wells G, Shea B, Shea B, O'Connell D, Peterson J, et al., editors. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomised Studies in Meta-Analyses2014. | ||||
| 28. Agarwal S, Melmed K, Dogra S, Jain R, Conway J, Galetta S, et al. Increase in Ventricle Size and the Evolution of White Matter Changes on Serial Imaging in Critically Ill Patients with COVID-19. Neurocrit Care. 2021;35(2):491-500. https://doi.org/10.1007/s12028-021-01207-2 PMid:33674942 PMCid:PMC7935478 |
||||
| 29. Ammar A, Distinguin L, Chetrit A, Safa D, Hans S, Carlier R, et al. Transient modifications of the olfactory bulb on MR follow-up of COVID-19 patients with related olfactory dysfunction. J Neuroradiol. 2022;49(4):329-32. https://doi.org/10.1016/j.neurad.2022.03.003 PMid:35306004 PMCid:PMC8926438 |
||||
| 30. Del Brutto OH, Mera RM, Costa AF, Rumbea DA, Recalde BY, Castillo PR. Long coronavirus disease-related persistent poor sleep quality and progression of enlarged perivascular spaces. A longitudinal study. Sleep. 2022;45(9). https://doi.org/10.1093/sleep/zsac168 PMid:35878737 PMCid:PMC9384510 |
||||
| 31. Douaud G, Lee S, Alfaro-Almagro F, Arthofer C, Wang C, McCarthy P, et al. SARS-CoV-2 is associated with changes in brain structure in UK Biobank. Nature. 2022;604(7907):697-707. https://doi.org/10.1038/s41586-022-04569-5 PMid:35255491 PMCid:PMC9046077 |
||||
| 32. Hellgren L, Birberg Thornberg U, Samuelsson K, Levi R, Divanoglou A, Blystad I. Brain MRI and neuropsychological findings at long-term follow-up after COVID-19 hospitalisation: an observational cohort study. BMJ Open. 2021;11(10):e055164. https://doi.org/10.1136/bmjopen-2021-055164 PMid:34706965 PMCid:PMC8551746 |
||||
| 33. Ippolito A, Urban H, Ghoroghi K, Rosbach N, Lingwal N, Adam EH, et al. Prevalence of acute neurological complications and pathological neuroimaging findings in critically ill COVID-19 patients with and without VV-ECMO treatment. Sci Rep. 2022;12(1):17423. https://doi.org/10.1038/s41598-022-21475-y PMid:36261436 PMCid:PMC9579632 |
||||
| 34. Kas A, Soret M, Pyatigoskaya N, Habert MO, Hesters A, Le Guennec L, et al. The cerebral network of COVID-19-related encephalopathy: a longitudinal voxel-based 18F-FDG-PET study. Eur J Nucl Med Mol Imaging. 2021;48(8):2543-57. https://doi.org/10.1007/s00259-020-05178-y PMid:33452633 PMCid:PMC7810428 |
||||
| 35. Lersy F, Bund C, Anheim M, Mondino M, Noblet V, Lazzara S, et al. Evolution of Neuroimaging Findings in Severe COVID-19 Patients with Initial Neurological Impairment: An Observational Study. Viruses. 2022;14(5). https://doi.org/10.3390/v14050949 PMid:35632691 PMCid:PMC9145920 |
||||
| 36. Salomon T, Cohen A, Barazany D, Ben-Zvi G, Botvinik-Nezer R, Gera R, et al. Brain volumetric changes in the general population following the COVID-19 outbreak and lockdown. Neuroimage. 2021;239:118311. https://doi.org/10.1016/j.neuroimage.2021.118311 PMid:34182098 |
||||
| 37. Tian T, Wu J, Chen T, Li J, Yan S, Zhou Y, et al. Long-term follow-up of dynamic brain changes in patients recovered from COVID-19 without neurological manifestations. JCI Insight. 2022;7(4). https://doi.org/10.1172/jci.insight.155827 PMid:35191397 PMCid:PMC8876627 |
||||
| 38. Miners S, Kehoe PG, Love S. Cognitive impact of COVID-19: looking beyond the short term. Alzheimer's Research & Therapy. 2020;12(1):170. https://doi.org/10.1186/s13195-020-00744-w PMid:33380345 PMCid:PMC7772800 |
||||
| 39. Sachdev A, Amanullah S. Covid-19 Analysis: Is there an Association Between Covid-19 and Development of Cognitive Deficits? Clin Neuropsychiatry. 2022;19(5):328-34. | ||||
| 40. Huang S, Zhou Z, Yang D, Zhao W, Zeng M, Xie X, et al. Persistent white matter changes in recovered COVID-19 patients at the 1-year follow-up. Brain. 2021;145(5):1830-8. https://doi.org/10.1093/brain/awab435 PMid:34918020 PMCid:PMC8754808 |
||||
| 41. Agrawal S, Farfel JM, Arfanakis K, Al-Harthi L, Shull T, Teppen TL, et al. Brain autopsies of critically ill COVID-19 patients demonstrate heterogeneous profile of acute vascular injury, inflammation and age-linked chronic brain diseases. Acta Neuropathol Commun. 2022;10(1):186. https://doi.org/10.1186/s40478-022-01493-7 PMid:36528671 PMCid:PMC9758667 |
||||
| 42. Almutairi MM, Sivandzade F, Albekairi TH, Alqahtani F, Cucullo L. Neuroinflammation and Its Impact on the Pathogenesis of COVID-19. Front Med (Lausanne). 2021;8:745789. https://doi.org/10.3389/fmed.2021.745789 PMid:34901061 PMCid:PMC8652056 |
||||
| 43. Spudich S, Nath A. Nervous system consequences of COVID-19. Science. 2022;375(6578):267-9. https://doi.org/10.1126/science.abm2052 PMid:35050660 |
||||
| 44. Klein R, Soung A, Sissoko C, Nordvig A, Canoll P, Mariani M, et al. COVID-19 induces neuroinflammation and loss of hippocampal neurogenesis. Res Sq. 2021. https://doi.org/10.21203/rs.3.rs-1031824/v1 |
||||
| 45. Najt P, Richards HL, Fortune DG. Brain imaging in patients with COVID-19: A systematic review. Brain Behav Immun Health. 2021;16:100290. https://doi.org/10.1016/j.bbih.2021.100290 PMid:34230916 PMCid:PMC8249107 |
||||
| 46. Li Q, Dang C, Wang L-H. Neuroinflammation in mild respiratory COVID-19: insights into cognitive impairment in milder cases. Military Medical Research. 2022;9(1):72. https://doi.org/10.1186/s40779-022-00431-x PMid:36539855 PMCid:PMC9763786 |
||||
| Article View | 1,177 |
| PDF Download | 531 |